










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.1 Lisboa mar. 2017
ORIGINAL ARTICLE
Are cranberry capsules effective and safe in preventing urinary tract infections in kidney transplantation? A randomized pilot clinical trial.
Tiago Assis Pereira1, Ana Raquel Fernandes2, Artur Mendes1, Regina Oliveira1, Ana Casqueiro1, Rita Birne1, Patrícia Matias1, Cristina Jorge1, Teresa Adragão1, Margarida Bruges1, Cristina Toscano3, Tânia Laranjeira4, Ana Mirco4, Fátima Falcão4, Domingos Machado1, André Weigert1
1 Department of Nephrology, Hospital Santa Cruz, Carnaxide, Portugal
2 Department of Nephrology, Hospital São Bernardo, Setúbal, Portugal
3 Microbiology Laboratory, Hospital Egas Moniz, Lisboa
4 Hospital Pharmacy, Hospital Santa Cruz, Carnaxide, Portugal
ABSTRACT
Introduction: Kidney transplant (KT) recipients are highly susceptible to urinary tract infections (UTIs). Few data are available regarding the effects of cranberry products in KT recipients. Subjects and methods: This was a randomized double-blind study comparing daily treatment with a cranberry capsule versus a placebo capsule for 6 months. The study protocol was conducted in accordance with the Helsinki Declaration and was approved by the local ethics committee. The study group comprised women undergoing KT for over 1 year, and the exclusion criteria included simultaneous antibiotic UTI prophylaxis. The primary endpoint was UTI occurrence, and the secondary endpoints were the time to first UTI, hospitalization, antibiotic resistance, graft function, immunosuppressive dose changes, and side effects. Results: 55 KT women at a single centre were included as follows: 25 were randomized to the cranberry group, and 30 were assigned to the placebo group. During the study period, 16.4% of the participants presented with a UTI. A diagnosis of UTI within the previous year and KT duration, but not cranberry use (p=0.95) were independent predictors of UTI. Discussion: Cranberry capsules appear to be safe in KT women; however, no clinical efficacy of UTI prophylaxis was demonstrated in this well-designed but underpowered study. Further multicentric and longer trial should be performed to determine cranberry clinical efficacy.
Key-words: Cranberry; Prophylaxis; Kidney Transplantation; Urinary Tract Infection; Vaccinium macrocarpon.
INTRODUCTION
Urinary tract infections (UTIs) are a critical burden in kidney transplant (KT) recipients1-3. Cranberry, or Vaccinium macrocarpon, is a fruit with an extract that is used as traditional UTI prophylaxis. Alongside the apparent benefit of cranberry extract to UTI prevention, there is a clear perception that relevant adverse effects are rare.4
However, scarce evidence is available concerning the efficacy and safety of cranberry products in KT patients.
We performed a randomized, double-blind placebocontrolled study to evaluate the efficacy and safety of cranberry capsules in women who had received a KT. To our knowledge, this is the first randomized study conducted to assess the potential benefit and safety of cranberry treatment in the prevention of UTIs in KT.
SUBJECTS AND METHODS
Study design and subjects
This was a randomized, double-blind, placebo-controlled study comparing daily placebo or cranberry capsule administration for a total of 6 months in a Kidney Transplant Unit – Unidade de Transplantação António Pina, Hospital Santa Cruz, Centro Hospitalar Lisboa Ocidental (CHLO). The study protocol and consent form were approved by the Ethics Committee at the CHLO, and research was conducted according to the principles expressed in the Declaration of Helsinki. Study subjects were adult women who had received a KT more than 12 months earlier, had an estimated glomerular filtration rate ≥ 30 mL/min/1.72 m2, and had received no other pharmacological prophylaxis treatment during the study. Exclusion criteria included the presence of an indwelling catheter, pregnancy, UTI diagnosis or suspicion of UTI at the time of screening, use of long-term antibiotics or cranberry products, and a know intolerance or allergy to cranberry products.
Primary outcome
The primary outcome was UTI occurrence during the study period.
Secondary outcomes
The time from randomization to UTI diagnosis, antibiotic resistance profile changes, pharmacological interactions with immunosuppressive drugs, graft function evolution, tolerability, and safety were evaluated.
Study product
The pharmaceutical company Xamane® manufactured and supplied both the cranberry and placebo capsules. Cranberry capsules were approved and available as over-the-counter medication and each capsule contained 36 mg of A-type proanthocyanidins and 100 mg of ascorbic acid. The placebo capsule consisted of 100 mg of ascorbic acid. Both capsules were indistinguishable and codified to enable double-blinding.
Sample size
Estimating that UTI would occur in 30% of patients and based on a previous study by Pagonas et al., we predicted that a final sample of 140 participants would be required to have 80% power at p<0.05 of detecting a 60% UTI reduction in the cranberry capsule treatment group.5
Randomization
Using a computer-generated randomization table, subjects were randomized to receive either cranberry or placebo.
Collected variables
Socio-demographic characteristics, cause of kidney disease and co-morbidities were recorded.
Patients were further characterized according to the induction and maintenance immunosuppression.
Patients were divided into high and low immunologic risk groups according to the induction regimen (antithymocyte globulin or basiliximab, respectively).
To characterize and compare UTI risk, UTI occurrence during the 12-month period prior to study inclusion was evaluated.
Follow-up and adherence
All patients underwent follow-up clinic visits and laboratory evaluations, including urinalysis, urine cultures, and serum levels of immunosuppressive medication, according to the KT centre clinical practice protocols.
Statistical analysis
All statistical analyses were performed using SPSS® version 21.0 software, according to the intentionto-treat principle and a two-sided p<0.05 value was considered statistically significant. Baseline sociodemographic and clinical characteristics were summarized using descriptive statistics. According to the nature and distribution of data, variables were compared using the chi-square test, Fishers exact test, Students t-test, and Mann-Whitney U test, as appropriate.
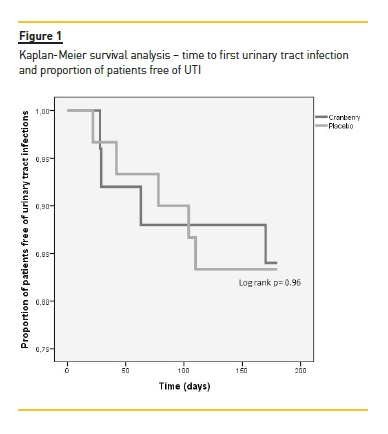
Time to the first episode of infection was plotted as a Kaplan-Meier curve, and differences were assessed using the log rank test. Multivariate logistic regression analysis was used to evaluate independent risk factors associated with UTI during the study period.
RESULTS
Fifty-five women with KT were recruited: 25 were randomized to receive cranberry capsules, and 30 were randomized to receive placebo capsules. The different number of randomized patients in each group is the result of a randomization table designed for a larger sample and the inability to reach a larger sample size.
Socio-demographic variables and clinical characteristics
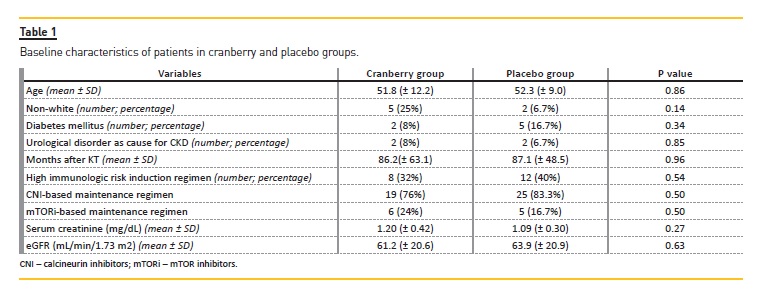
Table 1 lists the baseline socio-demographic and clinical characteristics of the included patients. A global analysis indicated a relatively lower proportion of diabetic patients (12.7%) and patients with previous urological disorders that led to chronic kidney disease (CKD) (7.2%).
Urinary tract infections
Previous 12-month period and risk factors
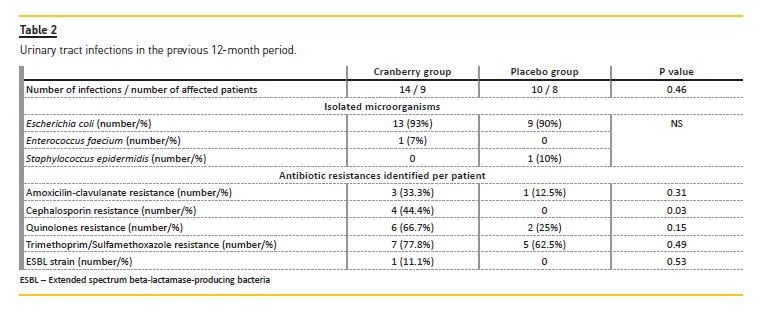
Twenty-four cases of UTI were diagnosed in 17 patients (30.9%). The leading causative microorganism responsible for UTI in this population was Escherichia coli (n = 22, 91.7%). A significant difference in cephalosporin resistance was identified, and the resistance was greater in the cranberry group. Table 2 lists UTI occurrence and microbiological data in both groups.
Age, race, diabetes mellitus, previous urological disorder, date of KT, maintenance regimen, and graft function were not associated with a higher UTI incidence.
Urinary tract infections during the study
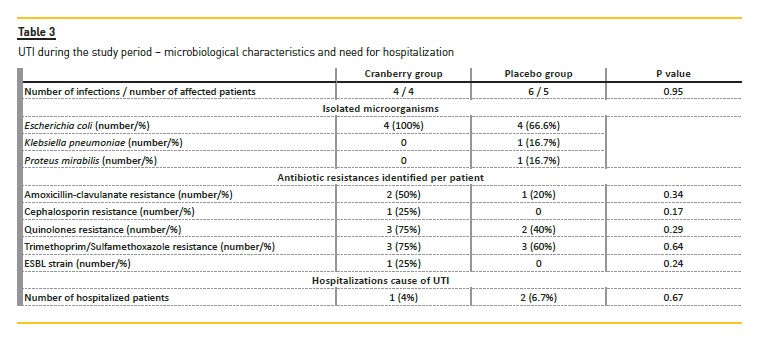
During the 6-month study period, 9 patients (16.4%) presented with 10 UTIs, 4 patients in the cranberry group (16%) and 5 patients in the placebo group (16.7%) (p = 0.95). Antimicrobial resistance rates of identified bacteria and hospitalizations due to UTI are presented in Table 3. The only factors associated with UTI during the study period were a diagnosis of UTI in the previous 12 months (p = 0.019) and KT duration (p = 0.012). After adjusting for age, diabetes mellitus diagnosis, and graft function, KT duration (p = 0.021; ExpB 1.02, 95% CI 1.003–1.035) and prior UTI (p = 0.028; ExpB 7.25, 95% CI 1.22-43.1) persisted as predictors of UTI occurrence during the study period. There was no difference in the risk of developing UTI between the groups after adjusting for KT duration and prior UTI (p = 0.62). After study inclusion, the global median time until UTI diagnosis was 63 days (IQ range 28.5–107 days), with no difference detected between the groups (p = 0.97). A Kaplan-Meier plot of UTI incidence showed a similar infection rate according to time (log-rank test p = 0.96), as noted in Figure 1. Cox regression analysis confirmed that KT duration and prior UTI were predictors for UTI during the study period (p = 0.009 and p = 0.015, respectively).
Immunosuppression interference
Patients exhibited adequate therapeutic levels of immunosuppressants in the blood, and immunosuppressant doses were adjusted during the study due to levels under or over the therapeutic goal in 8 patients (5 in cranberry group and 3 in placebo group).
Graft function and side effects
During the study period, there was a global mean serum creatinine decrease of -0.06 ± 0.16 mg/dL, which was not related to the intervention (p = 0.25) or to UTI occurrence (p = 0.20). No patient death, urinary tract obstruction, or graft loss was found in either group of patients. Four patients presented with adverse events, and one patient in the cranberry group abandoned the study due to disturbing epigastralgias. No serious adverse events or hospitalizations (due to causes other than UTI) occurred in either group.
DISCUSSION
Tract infections in kidney transplant patients
UTI is a common occurrence in the general population and is associated with considerable clinical and socioeconomic consequences.6 In patients who have undergone KT, UTI incidence is much higher, and the associated clinical and economic issues are exacerbated.7,8
Different immunosuppressive medications have been associated with different UTI rates in some studies.9
Contrary to these findings, the current study did not show such a finding.
Cranberry characteristics and potential benefits and harms
The efficacy of cranberry treatment as UTI prophylaxis is based on its effect on bacterial adherence in epithelial cells, primarily in the urinary tract. This action is essentially preventive and has no effect on displacing bacteria already attached to epithelial cells or interfering with the bacterial life cycle. Therefore, cranberry treatment can be used only for UTI prevention and not as a cure.10 Adherence to mucosal surfaces is a prerequisite for the development of most mammalian infections and is facilitated by fimbriae, which enable bacteria to resist cleansing mechanisms and overcome nutrient deprivation.11,12 Only a cranberry component, A-type proanthocyanidins (ATP), was capable of inhibiting P-fimbriae, which is primarily present in Escherichia coli.13 The evaluation of urinary antibacterial adhesion in in vitro and in vivo models revealed a significant reduction in bacterial adherence at an ATP dose of 36 mg or higher (efficacy steadily increased until the dose reached 108 mg).14 Other studies reported the inhibition of adherence and flagellum-mediated motility, and the potentiation of antibiotic activity for a wide range of microorganisms.
Importantly, the efficacy of ATP against bacteria is independent of the bacterial antibiotic resistance profile.15,16
Another mechanism of action of cranberry treatment for UTI prophylaxis is based on its effects on the colonic and vaginal tracts. ATP binds to pathogenic Escherichia isolates in these locations and inhibits bacterial adhesion prior to further introduction into the urinary tract.
As a consequence, ATP influences bacterial selection in these tracts to favour the survival of non-adherent, less pathogenic strains.15
Clinical studies have reported variable clinical effects associated with the use of cranberry products for UTI prophylaxis.17,18 A Cochrane renal group presented a meta-analysis followed by successive updates regarding the efficacy of cranberry products for UTI prophylaxis. The most recent updated Cochrane review included 24 studies, with a total of 4,473 patients. The comparison arms consisted of placebo, no treatment, water, methenamine hippurate, antibiotics, or lactobacillus. Overall, cranberry products were not associated with an increased benefit in the general population or in any of the subgroups. The quality of studies was considered good, but most of the studies were too small to enable a significant difference to be detected.17 The drawbacks of these reviews are that most studies did not report the amount of the active ingredient and there was a lack of uniformity regarding the intervention, including differences in cranberry formulation, dosing regimen, and duration of the intervention. Again, no KT recipients were included, reflecting a lack of studies in this population. A large number of dropouts and withdrawals (up to 55%) was detected in cranberry juice trials, which was attributed to the reduced lower palatability/acceptability of the cranberry juice.19
The newer capsule and tablet formulations of cranberry extract have been evaluated and comparison studies revealed equivalent efficacy as for juice. Furthermore, the capsule formulation is more convenient, is less expensive and overcomes compliance issues.4
Urinary tract infection prophylaxis in patients with a kidney transplant
UTI management remains a widely studied topic in the field of kidney transplantation. Contrary to findings in the general population, no conclusive data are available on antibiotic or non-antibiotic prophylaxis modalities in KT patients. Retrospective data concerning this subject demonstrate that antibiotic prophylaxis decreased UTI occurrence and hospitalization rates.
However, long-term results and prospective trials addressing a loss of efficacy and an enhanced risk of antimicrobial resistance are lacking.20 The only published study on UTI prophylaxis in KT patients with cranberry products was a retrospective trial that included 82 KT recipients with frequent UTI. Compared with placebo, cranberry juice was associated with a significant reduction in the annual incidence of UTI by 63.9% (p<0.001).5
The current study is the first randomized doubleblind placebo controlled trial to evaluate the efficacy of cranberry treatment as UTI prophylaxis in KT recipients.
We decided to include only female KT due to the increased susceptibility to UTI in females.1,7,21,22 The use of a cranberry capsule in this study provided a uniform method of distributing the product. Additionally, the use of a capsule made it possible to use a similar placebo capsule to achieve double blindness. Regarding primary and secondary endpoints, treatment with cranberry was not associated with fewer UTI events or an increased time to develop the first UTI, and we found no differences in microbiological profiles.
Immunosuppressive therapy interference and graft function were not affected by treatment with cranberry.
These particular topics were addressed for the first time in the current study, as no previously published studies evaluated the potential effects of cranberry in a KT setting.
Limitations
The main limitations of this trial are the small group size and short follow-up, rendering this study underpowered to detect a difference between the effects of cranberry and placebo. UTI rates were lower in the current study than those assumed in the original power calculations. We propose that the patients included in the current study represent a lower-risk sub-group, as diabetes mellitus prevalence was low, current urological disorders were absent, and graft function was normal.
Given the previous 12-month UTI incidence observed, we would have required 76 participants per group to have 80% power of detecting a difference at p = 0.05 at 12 months.
In an attempt to exclude potential effects of concomitant antibiotic use and to eliminate potential bias, we decided to exclude patients with a history of frequent UTIs who were receiving chronic antibiotic therapy.
Thus, we excluded patients who would benefit more from additional preventive measures and who present with a higher event incidence.
Another explanation for the lower efficacy is the cranberry dosage used in this study, which may have been insufficient for prophylaxis in this specific population.
Studies have demonstrated that a minimum dose of 36 mg of ATP is needed for UTI prophylaxis; however, efficacy is dose-dependent, suggesting that higher doses can be more protective.23
Ascorbic acid (AA) is an essential micronutrient that is naturally present in foods, and high levels are present in cranberry. In the current study, it was present in both the cranberry and placebo capsules at the same dose (100 mg)16,24 One of the reasons for the use of AA is the stabilization of cranberry extract. Additionally, other studies evaluating cranberry juices vs placebo also included AA in both products.25,26 However, AA has been suggested to prevent UTI in experimental studies by pH-dependent and pH-independent mechanisms.27,28 We speculate that AA consumption in both groups could lead to a global reduction in UTI incidence.
CONCLUSION
We investigated the ability of cranberry to reduce UTI incidence in KT patients, an understudied population.
In addition to the absence of clinical efficacy of UTI prophylaxis, this study indicates that treatment with cranberry capsules can be a simple and safe approach in KT care. Additional larger and longer studies should be performed.
References
1. Gołe¸biewska J, De¸bska-Ślizień A, Komarnicka J, et al. Urinary tract infections in renal transplant recipients. Transplant Proc. 2011;43:2985-90. [ Links ]
2. Pellé G, Vimont S, Levy PP, H et al. Acute pyelonephritis represents a risk factor impairing long-term kidney graft function. Am J Transplant. 2007;7:899-907. [ Links ]
3. Valera B, Gentil MA, Cabello V, Fijo J, Cordero E, Cisneros JM. Epidemiology of urinary infections in renal transplant recipients. Transplant Proc. 2006;38:2414-5. [ Links ]
4. Wang C, Fang C, Chen N, et al. Cranberry-containing products for prevention of urinary tract infections in susceptible populations: a systematic review and meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:988-96. [ Links ]
5. Pagonas N, Hörstrup J, Schmidt D, et al. Prophylaxis of recurrent urinary tract infection after renal transplantation by cranberry juice and L-methionine. Transplant Proc. 2012;44:3017-21. [ Links ]
6. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-60. [ Links ]
7. Bispo A, Fernandes M, Toscano C, Marques T, Machado D, Weigert A. Infeções do trato urinario numa coorte de transplantados renais. Acta Med Port. 2014;27:364-71. [ Links ]
8. Golebiewska J, Debska-Slizien A, Rutkowski B. Urinary tract infections during the first year after renal transplantation: one centers experience and a review of the literature. Clin Transplant. 2014;28:1263-70. [ Links ]
9. Alangaden G, Thyagarajan R, Gruber S, et al. Infectious complications after kidney transplantation: current epidemiology and associated risk factors. Clin Transplant. 2006;20:401-9. [ Links ]
10. Harkins K. Whats the use of cranberry juice? Age Ageing. 2000;29:9-12. [ Links ]
11. Zafriri D, Oron Y, Eisenstein BI, Ofek I. Growth advantage and enhanced toxicity of Escherichia coli adherent to tissue culture cells due to restricted diffusion of products secreted by the cells. J Clin Invest. 1987;79:1210-6. [ Links ]
12. Beachey E. Bacterial adherence: adhesin-receptor interactions mediating the attachment of bacteria to mucosal surface. J Infect Dis. 1981;143:325-45. [ Links ]
13. Plos K, Connell H, Jodal U, et al. Intestinal carriage of P fimbriated Escherichia coli and the susceptibility to urinary tract infection in young children. J Infect Dis. 1995; 171:625-31. [ Links ]
14. Lavigne J, Bourg G, Combescure C, Botto H, Sotto A. In-vitro and in-vivo evidence of dose-dependent decrease of uropathogenic Escherichia coli virulence after consumption of commercial Vaccinium macrocarpon (cranberry) capsules. Clin Microbiol Infect. 2008;14:350-5. [ Links ]
15. Gupta K, Chou M, Howell A, Wobbe C, Grady R, Stapleton A. Cranberry products inhibit adherence of p-fimbriated Escherichia coli to primary cultured bladder and vaginal epithelial cells. J Urol. 2007;177:2357-60. [ Links ]
16. Guay D. Cranberry and urinary tract infections. Drugs. 2009;69:775-807. [ Links ]
17. Jepson R, Williams G, Craig J. Cranberries for preventing urinary tract infections. Cochrane database Syst Rev. 2012;CD001321. [ Links ]
18. Vasileiou I, Katsargyris A, Theocharis S, Giaginis C. Current clinical status on the preventive effects of cranberry consumption against urinary tract infections. Nutr Res. 2013;33(8):595-607. [ Links ]
19. Jepson R, Craig J, Williams G. Cranberry products and prevention of urinary tract infections. JAMA. 2013;310:1395-6. [ Links ]
20. Chuang P, Parikh C, Langone A. Urinary tract infections after renal transplantation: a retrospective review at two US transplant centers. Clin Transplant. 2005;19:230-5. [ Links ]
21. Ariza-Heredia E, Beam E, Lesnick T, Kremers WK, Cosio F, Razonable R. Urinary tract infections in kidney transplant recipients: role of gender, urologic abnormalities, and antimicrobial prophylaxis. Ann Transplant. 2013;18:195-204. [ Links ]
22. Camargo L, Esteves A, Ulisses L, Rivelli G, Mazzali M. Urinary tract infection in renal transplant recipients: incidence, risk factors, and impact on graft function. Transplant Proc. 2014;46:1757-9. [ Links ]
23. Howell A, Botto H, Combescure C, et al. Dosage effect on uropathogenic Escherichia coli anti-adhesion activity in urine following consumption of cranberry powder standardized for proanthocyanidin content: a multicentric randomized double blind study. BMC Infect Dis. 2010;10:94. [ Links ]
24. Baxmann A, Mendonça C, Heilberg I. Effect of vitamin C supplements on urinary oxalate and pH in calcium stone-forming patients. Kidney Int. 2003;63:1066-71. [ Links ]
25. Avorn J, Monane M, Gurwitz J, Glynn R, Choodnovskiy I, Lipsitz L. Reduction of bacteriuria and pyuria after ingestion of cranberry juice. JAMA. 1994;271:751-4. [ Links ]
26. McMurdo M, Bissett L, Price R, Phillips G, Crombie IK. Does ingestion of cranberry juice reduce symptomatic urinary tract infections in older people in hospital? A double-blind, placebo-controlled trial. Age Ageing. 2005;34:256-61. [ Links ]
27. Carlsson S, Wiklund N, Engstrand L, Weitzberg E, Lundberg JO. Effects of pH, nitrite, and ascorbic acid on nonenzymatic nitric oxide generation and bacterial growth in urine. Nitric Oxide. 2001;5:580-6. [ Links ]
28. Ochoa-Brust G, Fernández A, Villanueva-Ruiz G, Velasco R, Trujillo-Hernández B, Vásquez C. Daily intake of 100 mg ascorbic acid as urinary tract infection prophylactic agent during pregnancy. Acta Obstet Gynecol Scand. 2007;86:783-7. [ Links ]
Tiago Assis Pereira, MD,
Department of Nephrology,
Hospital Santa Cruz, Carnaxide, Portugal.
E-mail: Tiago_assis_pereira@yahoo.com
Disclosure of potential conflicts of interest: none declared
ACKNOWLEDGMENTS
The authors are greatly indebted to the nursing staff for contributing to the study and to Xamane® for donating the cranberry and placebo capsules.
DISCLOSURE
Xamane® supplied the placebo and cranberry capsules. Xamane® had no role in the design; methods; subject recruitment; data collection, analysis, and interpretation; decision to submit the manuscript for publication; or preparation of the manuscript.
All authors declare no financial support of incentive for performance, submission and publication of this manuscript.
Tiago Assis Pereira participated in the study design and patient recruitment and wrote the manuscript; Raquel Fernandes participated in the database development, data collection, and analysis; Artur Mendes led the statistical analysis; the nurses helped with patient recruitment, compliance, and verification of side effects; Cristina Toscano coordinated the microbiological surveillance; Tânia Laranjeira, Ana Mirco, and Fátima Falcão coordinated the capsule supply, monitored adherence, and registered side effects; Domingos Machado provided central assistance with the development of study protocols and project coordination; André Weigert led the study concept, design, and coordination and funding acquisition efforts and participated in manuscript revision; and the other authors participated in the study design, patient recruitment, and manuscript revision.
All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Abbreviations:
Kidney Transplant – KT
Urinary Tract Infection – UTI
Centro Hospitalar Lisboa Ocidental – CHLO
Chronic Kidney Disease – CKD
A-type proanthocyanidins – ATP
Trimethoprim/sulfamethoxazole – TMP/SMZ
Ascorbic acid – AA
Received for publication: Sep 22, 2016
Accepted in revised form: Jan 31, 2017


{kind=link}
{kind=link}
{kind=link}