










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.30 no.3 Lisboa set. 2016
CASE REPORT
Fever of unknown origin and pericardial effusion in a haemodialysis patient
Tiago Assis Pereira1, Margarida Gonçalves1, João Torres1, Ilídio Rodrigues1, Ana Pires2, Helena Boquinhas1, José Barata1
1 Department of Nephrology, Hospital Santa Cruz, Carnaxide, Portugal
2 Unidade Linda‑a‑Velha, Diaverum Portugal, Linda‑a‑Velha, Portugal.
ABSTRACT
Introduction: Retroperitoneal fibrosis is a rare disorder. The idiopathic (IRF) form of the disease accounts for most of cases. Renal failure is a common finding, and some patients present with non-functioning kidneys, as a result of long-lasting obstructive uropathy. The symptoms and signs associated with IRF are non-specific and, thus, its diagnosis requires a high degree of suspicion. Case Report: A 71-year-old man with multifactorial chronic kidney disease required initiation of haemodialysis on February 2014, due to disease progression to end-stage renal disease (ESRD). His past medical history included the diagnosis of optic neuritis, seronegative arthritis and biopsy-proven retroperitoneal fibrosis. The patient had been treated with glucocorticoids for 13 years, stopping this treatment at the time of haemodialysis (HD) initiation. Two months after initiation of HD, in April 2014, the patient complained of malaise and presented with recurrent fever. A thorough clinical and laboratory evaluation was unremarkable. An echocardiogram showed a minor to moderate pericardial effusion that led to prescription of HD intensification. Five months later, he was admitted to the Hospital due to worsening of the pericardial effusion, requiring pericardiocentesis. Pericardial fluid analysis showed exudative changes. A thorough laboratory evaluation was performed and only interferon gamma release assay (IGRA) was positive. Empirical anti-bacillary therapy was initiated, waiting for definite mycobacterial cultures. One month later, as the patient maintained complains of malaise and fatigue, and had recurrent fever, he was readmitted to the Hospital. Mycobacterial cultures ultimately became negative. Further work-up was performed, including positron emission tomography/computed tomography (PET/CT) scan, which detected recurrence of IRF along with aortic, pericardial and pleural involvement. Following initiation of glucocorticoid treatment, a clinical and laboratoryl improvement was documented, that persisted at 11 months of follow-up. Conclusion: IRF is characterized by a relapsing nature, and clinical presentation includes local and systemic symptoms and complications, making it difficult to diagnose. Treatment of IRF is often delayed because of difficulties in reaching the correct diagnosis.
Key-Words: Fever of unknown origin; hemodialysis; idiopathic retroperitoneal fibrosis.
INTRODUCTION
Retroperitoneal fibrosis (RF) is a rare disease characterized by a chronic inflammation of periaortic retroperitoneum and subsequent fibrosis that extends to the surrounding tissues. Therefore this process may result in local organs entrapment and dysfunction. Ureter involvement can lead to renal insufficiency, which is a complication often present at the time of diagnosis1,2.
Retroperitoneal fibrosis may be idiopathic (RFI), corresponding to about two-thirds of cases, or secondary (due to inflammatory, malignant, infectious conditions, drugs, post-surgical or radiation therapy)1-3. The IgG4-related retroperitoneal fibrosis, a specific condition often associated with other autoimmune diseases (e.g., pancreatitis, prostatitis, sclerosing cholangitis and sialadenitis), is characterized by a higher recurrence rate4,5. This entity is characterized by extensive IgG4-positive plasma cell and T-lymphocyte infiltration of various organs.
The main clinical features of retroperitoneal fibrosis are abdominal and/or back pain which may be accompanied by constitutional symptoms (malaise, fever and weight loss), and an increase in serum inflammatory markers1,2,6.
The presence of retroperitoneal fibrosis in biopsyspecimens is generally considered the gold standard for the diagnosis of retroperitoneal fibrosis. However, imaging tests, such as computed tomography (CT) and magnetic resonance imaging (MRI) scans may provide crucial information to guide the diagnosis and detect possible secondary causes. To date, no specific diagnostic serum markers were identified. Since it is an active metabolic disease, positron emission tomography (PET) scan with 18-fluorodeoxyglucose in conjugation with CT (PET/CT) scan has been increasingly used for the diagnosis and monitoring of this condition2,7-11.
There is currently no consensus on the appropriate management of patients with retroperitoneal fibrosis, because no controlled therapeutic trials have been performed.
The treatment of IRF differs from the secondary form. While, in the latter, the treatment is directed toward its underlying cause, in IRF treatment includes glucocorticoids or other immunosuppressive medications. In both forms of the disease, surgical treatment may be required to deal with local complications (e.g., ureteral obstruction and intestinal occlusion). Glucocorticoids is the mainstay of immunosuppression in the idiopathic form. However, there are no guidelines regarding optimal dosage and duration of therapy, although most physicians would recommend at least a 3-month treatment. Other immunosuppressive medications, such as azathioprine, cyclophosphamide, methotrexate, cyclosporine, mycophenolate mofetil and colchicine, have been used to treat this condition, but only few studies suggest a beneficial effect12-17. Anecdotal reports on tamoxifen use in IRF, based on its anti-proliferative and anti-fibrotic properties, have also been published18,19.
In IRF, early diagnosis and early treatment (medical, surgical or both) are usually associated with good renal and patient long-term survival15,20. Recurrence occurs more often within the first 5 years following diagnosis and, thus, disease monitoring is mandatory. Clinical, laboratory (serum inflammatory markers) and routine imaging evaluations (ultrasound and CT scan) are used for disease monitoring, but their value is limited by the low specificity. Limited experience suggests that PET/CT and MRI scans may be useful tools (discriminating residual structural lesions from active disease lesions) for the management of IRF, although as far as PET/CT is concerning, its use in clinical practice is limited by economic constraints and equipment availability2,11.
In patients on haemodialysis, IRF is a rare disorder with a clinical presentation that includes both local and systemic symptoms and complications making difficult its diagnosis. In this case, treatment of IRF was delayed because of difficulties in reaching the correct diagnosis.
CASE REPORT
We report a case of IRF recurrence in a Caucasian 71-year-old male on maintenance haemodialysis. His prior medical history included the diagnoses of optic neuritis (at 58 years old), seronegative arthritis (at 64) and biopsy-proven IRF (at 65). The latter diagnosis was made after recurrent episodes of backache, and fever.
An abdomen ultrasound and CT scan was requested at the time and suggested the diagnosis of IRF, which was confirmed by a retroperitoneal biopsy. The patient was treated with glucocorticoids uninterruptedly from the age of 58 years old till the date of initiation of haemodialysis (in February 2014, at the age of 71). Over this period of time he developed difficult-to-control arterial hypertension and vascular peripheral disease.
Chronic kidney disease was diagnosed by the age of 69 and was considered multifactorial due to the longstanding presence of arterial hypertension, and of IRF with unilateral kidney atrophy (renovascular disease was then excluded). At the time, the clinical picture was interpreted as renal involvement by IRF and the patient was, thus, submitted to unilateral ureteral stenting, which, however, did not prevent chronic kidney disease (CKD) progression to end-stage renal disease (ESRD). At the age of 71 years old haemodialysis treatment was initiated and glucocorticoids treatment was suspended. Two months following the initiation of haemodialysis, in April 2014, the patient presented at the dialysis unit complaining of malaise and with recurrent fever for unspecified duration. At the time, blood cultures were negative and an echocardiogram showed a minor-to-moderate pericardial effusion, and no valvular vegetations were detected. To exclude uraemic pericarditis, the haemodialysis treatment was intensified. During this period the patient remained clinically stable despite the recurrent fever episodes.
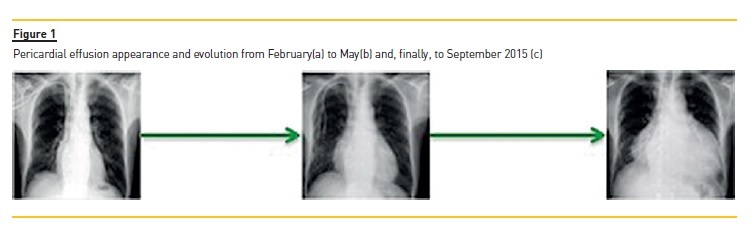
Five months later, in September 2014, patient was admitted to the Nephrology Department complaining of chest pain and fatigue for the last two weeks. Significant laboratory data included increased levels of inflammatory markers, and interferon gamma release assay (IGRA) was positive. Mantoux test, blood and pericardial effusion cultures autoimmune serology, and tumour markers were all negative. Chest radiography showed a marked increase in the cardiothoracic index (Fig. 1). Severe pericardial effusion was detected on transthoracic echocardiography and pericardiocentesis was performed. Pericardial fluid analysis showed an exudative pericardial fluid, where macrophages were the predominant cells, and low glucose and high lactate dehydrogenase levels.
Thoracic, abdominal and pelvic CT scan findings were unchanged from the previous admission (one year earlier) showing aortic and peri-aortic thickening, and these changes were interpreted as corresponding to residual fibrosis from IRF.
Given the positive IGRA test and the characteristics of the pericardial effusion, extra-pulmonary (pericardial) tuberculosis was tentatively diagnosed for which anti-bacillary therapy (isoniazid, rifampicin and pyrazinamide) was initiated, while waiting for definite mycobacterial cultures.
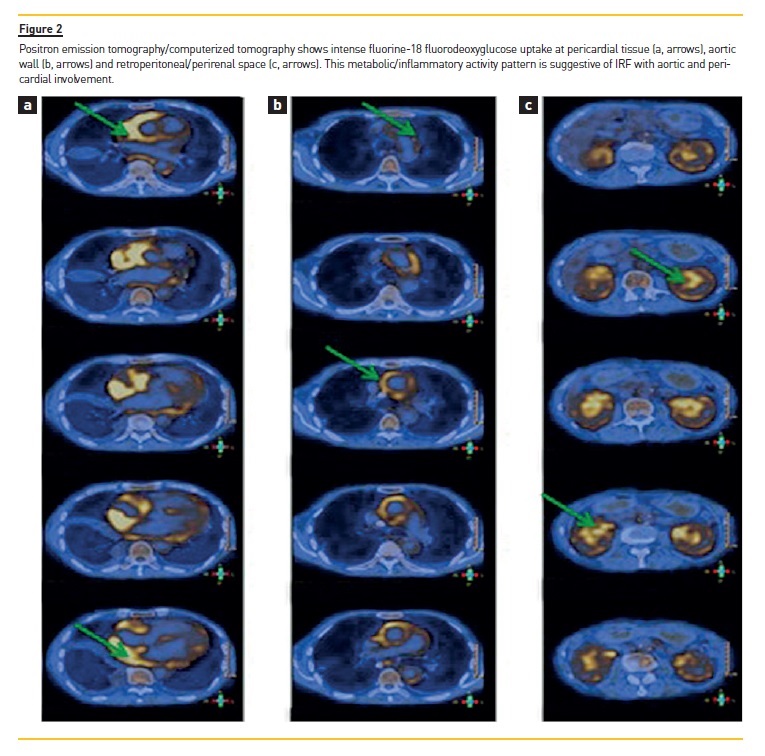
One month later, in October 2014, the patient was readmitted to the hospital due to persistence of the clinical picture (fatigue, malaise and sustained fever). Mycobacterial cultures collected one month earlier were negative. As no infectious or neoplastic disorder was found, the presence of IRF recurrence was suspected. Given the patients age, the fever and aortic involvement, a temporal artery biopsy was performed and excluded giant cell arthritis (GCA). A PET/CT scan revealed intense metabolic lesions in the kidneys, pleura, pericardium and aorta, and, thus, a diagnosis of IRF recurrence with aortic, pericardial and pleural involvement was made (Fig. 2). An IgG4 immunostaining of the original retroperitoneal biopsy was performed in order to exclude an immunoglobulin G4-related disease (IgG4-RD), and was unremarkable.
The patient was then treated with glucocorticoids, prednisolone 1 mg/Kg/day, following which there was a steady improvement in clinical and laboratory parameters.
Glucocorticoids were then progressively tapered to a minimum dose of 10mg per day of prednisolone.
After 11 months of therapy the patient remained clinically stable, without disease recurrence. Isoniazid was maintained as tuberculosis prophylaxis due to positive IGRA.
DISCUSSION
The diagnosis of IRF is difficult due to the rarity of this disorder and the fact that symptoms and signs are non-specific and, thus, its diagnosis requires a high degree of suspicion. Recurrence is common and is diagnosed by the clinical and radiological findings, but diagnosis is challenging in the ESRD population as clinical manifestations may be difficult to distinguish from uraemic symptoms and infectious diseases which are quite common in these patients. Additionally, urological obstruction is difficult to detect as most of these patients have a low residual renal function.
First-line imaging tests include ultrasonography and CT scan. However, these tests are not reliable for the diagnosis of IRF recurrence, as they cannot distinguish active from residual lesions. Therefore, the diagnosis of this disorder may require the use of MRI or PET/CT scan due to their additional potential for detecting and locating inflammatory activity2,7-11.
In ESRD patients, PET/CT scan may be safer than CT scan as it does not involve the use of radiographic contrast agents, but its use is limited by the high cost and scarce availability. Positron emission tomography is a radiological modality utilized in several medical settings, including in the diagnosis of oncologic, infectious and inflammatory disorders. As compared with CT scan, it has a higher diagnostic sensitivity and a more accurate ability to determine the disease extension and activity.
Gadolinium-based contrast agents used in MRI scans may lead to nephrogenic systemic fibrosis in ESRD patients. A possible alternative option is to perform an MRI scan without the use of gadolinium, which resolution is yet higher than that of CT. Data reporting MRI utility in IRF is extensive, including its use for diagnostic and therapeutic purposes. MRI presents higher specificity than CT scan, and can identify secondary causes2,7-11,21. To the best of our knowledge, there is no published data comparing PET scan with MRI scan in the diagnosis and monitoring of IRF.
In the present case, both PET/CT scan and MRI scan could be considered reasonable options for the diagnosis of IRF, but we opted to perform a PET/CT scan. It is, however, debatable whether MRI scan would be as conclusive as PET/CT scan was in diagnosing aortic, pericardial and pleural involvement.
In our case, the IRF recurrence diagnosis was delayed by 1) The atypical presentation of the clinical picture composed by pericardial effusion and prolonged fever; 2) High likelihood of other diagnostic hypotheses given the ESRD status and 3) Laboratory data suggesting the possibility of an infection with Kochs bacillus.
It should be noted that glucocorticoids were suspended after haemodialysis initiation because there was no signs of disease activity and the patient had completed a long course of glucocorticoids. Thus, it seems reasonable to suspect that glucocorticoids suspension was a precipitating factor of IRF recurrence.
Despite the use of several imaging and laboratory tests, only PET/CT provided additional information concerning the presence of inflammatory activity and the organs involved, confirming the potential advantages of this technique in this particular setting7,11,22-24. The aortic inflammation detected by PET/CT could be secondary to IRF or to large vessel vasculitis, such as GCA with aortic involvement. Although very rare, aortic and pericardial involvement in IRF has already been reported25. Giant cell arthritis was suspected in this case. The American College of Rheumatologys criteria for diagnosing GCA require the presence of three or more of the following: age > 50 years, new onset headache, abnormalities of the temporal arteries on palpation, ESR > 50 mm/hour, and abnormal temporal artery biopsy. Although in CGA temporal artery biopsy may be negative due to skip lesions, the patient did not meet this set of criteria.
Anecdotic reports described an association between GCA and retroperitoneal fibrosis26, and both diseases are equally treated by glucocorticoids as the first-line therapy27,28, suggesting that these are disorders of uncertain boundaries.
However, several questions remain unanswered: For how long should the patient be treated? How and when should we perform disease monitoring?
As a conclusion, IRF is characterized by a relapsing nature, and clinical presentation includes local and systemic symptoms and complications, making it difficult to diagnose. Treatment of IRF is often delayed because of difficulties in reaching the correct diagnosis.
References
1. Gilkeson GS, Allen NB. Retroperitoneal fibrosis. A true connective tissue disease. Rheum Dis Clin North Am 1996;22(1):23–38. [ Links ]
2. Vaglio A, Salvarani C, Buzio C. Retroperitoneal fibrosis. Lancet 2006;367(9506):241–251. [ Links ]
3. Corradi D, Maestri R, Palmisano A, et al. Idiopathic retroperitoneal fibrosis: clinicopathologic features and differential diagnosis. Kidney Int 2007;72(6):742–753. [ Links ]
4. Koo BS, Koh YW, Hong S, et al. Clinicopathologic characteristics of IgG4-related retroperitoneal fibrosis among patients initially diagnosed as having idiopathic retroperitoneal fibrosis. Mod Rheumatol 2014;7595:1–5. [ Links ]
5. Kamisawa T, Funata N, Hayashi Y, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol 2003;38(10):982–984. [ Links ]
6. Vivas I, Nicolás AI, Velázquez P, Elduayen B, Fernández-Villa T, Martínez-Cuesta A. Retroperitoneal fibrosis: Typical and atypical manifestations. Br J Radiol 2000;73(866):214–222. [ Links ]
7. Jansen I, Hendriksz TR, Han SH, Huiskes WL, van Bommel EF.18F-fluorodeoxyglucose position emission tomography (FDG-PET) for monitoring disease activity and treatment response in idiopathic retroperitoneal fibrosis. Eur J Intern Med 2010;21(3):216–221. [ Links ]
8. Moroni G, Castellani M, Balzani A, et al. The value of18F-FDG PET/CT in the assessment of active idiopathic retroperitoneal fibrosis. Eur J Nucl Med Mol Imaging 2012;39(10):1635–1642. [ Links ]
9. Caiafa RO, Vinuesa AS, Izquierdo RS, Brufau BP, Ayuso Colella JR, Molina CN. Retroperitoneal fibrosis: role of imaging in diagnosis and follow-up. Radiographics 2013;33(2):535–552. [ Links ]
10. Vaglio A, Greco P, Versari A, et al. Post-treatment residual tissue in idiopathic retroperitoneal fibrosis: active residual disease or silent scar? A study using 18F-fluorodeoxyglucose positron emission tomography. Clin Exp Rheumatol 2005;23(2):231–234. [ Links ]
11. Piccoli GB, Consiglio V, Arena V, et al. Positron emission tomography as a tool for the tailored management of retroperitoneal fibrosis: a nephro-urological experience. Nephrol Dial Transplant 2010;25(8):2603–2610. [ Links ]
12. Scheel PJ Jr, Feeley N, Sozio SM. Combined prednisone and mycophenolate mofetil treatment for retroperitoneal fibrosis: a case series. Ann Intern Med 2011;154(1):31–36. [ Links ]
13. Higgins PM, Bennett-Jones DN, Naish PF, Aber GM. Non-operative management of retroperitoneal fibrosis. Br J Surg 1988;75(6):573–577. [ Links ]
14. Kardar AH, Kattan S, Lindstedt E, Hanash K. Steroid therapy for idiopathic retroperitoneal fibrosis: dose and duration. J Urol 2002;168(2):550–555. [ Links ]
15. Moroni G, Gallelli B, Banfi G, Sandri S, Messa P, Ponticelli C. Long-term outcome of idiopathic retroperitoneal fibrosis treated with surgical and/or medical approaches. Nephrol Dial Transplant 2006;21(9):2485–2490. [ Links ]
16. Vega J, Goecke H, Tapia H, Labarca E, Santamarina M, Martínez G. Treatment of idiopathic retroperitoneal fibrosis with colchicine and steroids: a case series. Am J Kidney Dis 2009;53(4):628–637. [ Links ]
17. Swartz RD. Idiopathic retroperitoneal fibrosis: A review of the pathogenesis and approaches to treatment. Am J Kidney Dis 2009;54(3):546–553. [ Links ]
18. Van Bommel EF, Pelkmans LG, Van Damme H, Hendriksz TR. Long-term safety and efficacy of a tamoxifen-based treatment strategy for idiopathic retroperitoneal fibrosis. Eur J Intern Med 2013;24(5):444–450. [ Links ]
19. Clark CP, Vanderpool D, Preskitt JT. The response of retroperitoneal fibrosis to tamoxifen. Surgery 1991;109(4):502–506. [ Links ]
20. Li KP, Zhu J, Zhang JL, Huang F. Idiopathic retroperitoneal fibrosis (RPF): Clinical features of 61 cases and literature review. Clin Rheumatol 2011;30(5):601–605. [ Links ]
21. Salvarani C, Pipitone N, Versari A, et al. Positron emission tomography (PET): evaluation of chronic periaortitis. Arthritis Rheum 2005;53(2):298–303. [ Links ]
22. Magrey MN, Husni ME, Kushner I, Calabrese LH. Do acute-phase reactants predict response to glucocorticoid therapy in retroperitoneal fibrosis? Arthritis Rheum 2009;61(5):674–679. [ Links ]
23. Washino S, Hirai M, Matsuzaki A, Kobayashi Y.18F-Fluorodeoxyglucose positron emission tomography for diagnosis and monitoring of idiopathic retroperitoneal fibrosis associated with mediastinal fibrosis. Ann Nucl Med 2010;24(3):225–229. [ Links ]
24. Young PM, Peterson JJ, Calamia KT. Hypermetabolic activity in patients with active retroperitoneal fibrosis on F-18 FDG PET: report of three cases. Ann Nucl Med 2008;22(1):87–92. [ Links ]
25. Klisnick A, Fourcade J, Ruivard M, et al. Combined idiopathic retroperitoneal and mediastinal fibrosis with pericardial involvement. Clin Nephrol 1999;52(1):51–55. [ Links ]
26. Protopsaltis I, Sotiropoulos A, Foteinos A, et al. Chronic periaortitis (retroperitoneal fibrosis) concurrent with giant cell arteritis: a case report. J Med Case Rep 2014;8(1):167. [ Links ]
27. Hunder GG, Bloch DA, Michel BA, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 1990;33(8):1122–1128. [ Links ]
28. Davies CG, May DJ. The role of temporal artery biopsies in giant cell arteritis. Ann R Coll Surg Engl 2011;93(1):4–5. [ Links ]
Tiago Assis Pereira, M.D.
Department of Nephrology, Hospital Santa Cruz
Avenida Prof. Reinaldo dos Santos 2790-134 Carnaxide, Portugal.
E‑mail: Tiago_assis_pereira@yahoo.com
Disclosure of potential conflicts of interest: None declared
Received for publication: Nov 12, 2015
Accepted in revised form: Feb 2, 2016


{kind=link}
{kind=link}