










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.30 no.3 Lisboa set. 2016
ORIGINAL ARTICLE
Implications for patients waiting for a kidney transplant of using the calculated panel reactive antibody (cPRA)
Rita Magriço1,2, Jorge Malheiro1, Sandra Tafulo3, Sofia Pedroso1, Manuela Almeida1, La Salete Martins1, Leonídio Dias1, António Castro‑Henriques1, António Cabrita1
1 Departmento de Nefrologia e Transplante Renal do Hospital de Santo António do Centro Hospitalar do Porto
– Largo Professor Abel Salazar, 4099‑001 Porto
2 Serviço de Nefrologia do Hospital Garcia de Orta
– AvenidaTorrado da Silva, 2801‑951 Almada
3 Centro do Sangue e Transplantação do Porto, Instituto Português do Sangue e da Transplantação
– Rua Dr. Roberto Frias, 4200‑467 Porto
ABSTRACT
Introduction: Kidney transplant improves survival even in highly‑sensitized(HS) patients. To overcome their disadvantage in accessing transplantation, those with high Complement Dependent Cytotoxic PRA (CDC‑PRA) receive additional points during allocation. Whether this strategy reaches all HS patients and how long they wait for a transplant is largely undetermined. Methods: Patients on our units active wait‑list for kidney transplantation in the year 2014 were analyzed. CDC‑PRA and calculated PRA (cPRA) were recorded. To obtain cPRA, antibodies in the last serum available specific for HLA‑A,‑B or –DR with an intensity > 1000 MFI were considered. Results: The cPRA values in the population (N=551) were 0% (N=312), 1‑79% (N=118) and ≥ 80% (22%; N=121). Among these groups, the proportion of women (29.5, 55.9 and 61.2%, P<0.001), prior sensitizing events (43.3, 80.5 and 96.7%, P<0.001) and time on dialysis (median of 3.9, 4.1 and 6.0 years, P<0.001) increased with cPRA, respectively. In most of those with a cPRA ≥ 80%, the CDC‑PRA raised no suspicion of HS status (median 0%, P25‑75 0‑8%) and only 35 (28.9%) or 12 patients (9.9%) had a CDC‑PRA in the peak serum higher than 50 or 80%, respectively (cut‑offs needed to obtain additional points during allocation). HS patients by cPRA corresponded to 71% vs 15% of patients waiting for ≥ or <8 years, respectively (P<0.001). Even after exclusion of patients with a CDC‑PRA above 50%, this disproportionate representation remained (58% versus 13%, P<0.001). Conclusion: HS patients as measured by cPRA remained longer on the wait‑list, both in the primary analysis and when excluding those with a CDC‑PRA> 50%. Moreover, only 30% of HS by cPRA patients received the extra points designed to improve their transplantability. We consider that both CDC‑PRA and cPRA should be taken into account when defining HS status.
Key words: Allocation algorithm, Calculated PRA, Cytotoxic PRA, Highly sensitized patients, Kidney transplant, Waiting time.
INTRODUCTION
In end stage renal disease, kidney transplantation is associated with increased survival and improved quality of life when compared to remaining on dialysis1.
Since kidneys available for transplantation are scarce, there has been much debate regarding the ideal allocation system. An optimal system should maximize the chance of success of each transplant while giving all the candidates the same odds of being eligible for transplantation (balancing the principles of utility and justice)2.
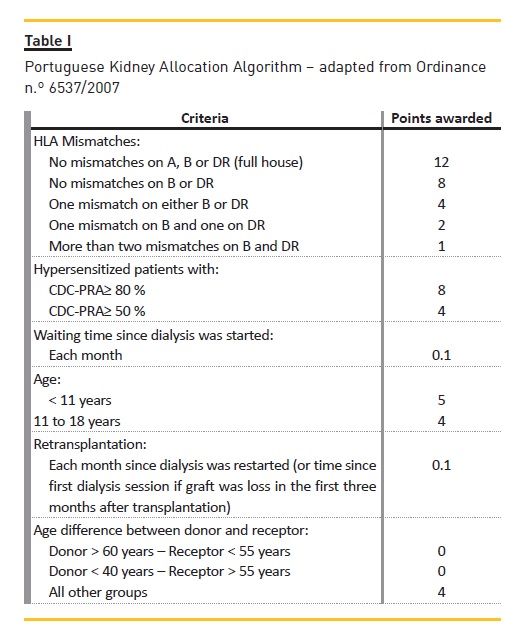
As established by Ordinance nº 6537/2007 (see Table I), the Portuguese allocation system takes into account time on dialysis and number of HLA compatibilities. Also, to compensate for the disadvantage that highly‑sensitized (HS) patients have in accessing transplantation, those with Complement Dependent Cytotoxic PRA (CDC‑PRA) ≥ 50 or 80% (common thresholds used to define HS status) are awarded extra points during kidney allocation.
Moreover, in patients with CDC‑PRA ≥ 80% it is not mandatory that donor and receptor have identical AB0 blood types; only AB0‑compatibility is required. Although in the 2007 Ordinance the selection of patients with CDC‑PRA ≥ 80% was made at a national level, since the publication of Ordinance nº11420/2008, their selection is made only regionally, which lowered the pool of donors available for these patients. In sum, the Portuguese allocation policy already aims to compensate for the disadvantage hypersensitized patients (HS) have in accessing transplantation, but so far only hypersensitized patients defined by CDC‑PRA ≥ 50% have access to special allocation criteria.
In order to clarify the results presented in this study,it is imperative to perform a brief review of four essential concepts: CDC‑PRA, calculated PRA, virtual cross‑match and cytotoxic cross‑match.
First, is must be remembered that CDC‑PRA and calculated PRA are performed prior to transplantation. They refer to the comparison of the anti‑HLA antibodies present in the candidate for kidney transplantation with the HLA phenotype of the population. Therefore, they aim to reflect the percentage of donors in the population who would not be immunologically compatible with the recipient,and hence the transplantability of each recipient.
When obtaining the Complement Dependent Cytotoxic Panel Reactive Antibody (CDC‑PRA) the serum of the candidate to kidney transplantation is put together with a panel of cells of different donors representative of the HLA phenotypes of the population. If the serum contains anti‑HLA antibodies capable of engaging a complement‑dependent cytotoxic (CDC) response, the cell with the correspondent HLA antigen becomes lysed.
The CDC‑PRA corresponds to the percentage of cells in the panel that become lysed and thus to the percentage of donors in the population against which the recipient would develop a CDC response. This CDC‑PRA is the one used by the current allocation algorithm in identifying hypersensitized candidates.
In contrast, to obtain the calculated PRA (cPRA), the serum of the candidate is screened for the presence of anti‑HLA antibodies, and antibodies specificities (identified by Luminex) are compared with the HLA phenotypes present in the population (estimated from the population of bone marrow donors1 or the population of previous kidney donors). The percentage of donors in the population against which the candidate has anti‑HLA antibodies is the cPRA3. The strength of each antibody present is also measured, in mean fluorescent intensity (MFI) units, and only antibodies with a MFI ≥ 1000 are considered in cPRA. No clear cPRA threshold has been determined in order to consider apatient HS, but most studies use the value ≥80%.
Whereas CDC‑PRA and cPRA are performed prior to transplantation and aim to determine the percentage of donors in the population who would not be immunologically compatible with the recipient, virtual and cytotoxic cross‑matches are performed after a specific donor becomes available and aim to avoid attributing a kidney to an HLA‑incompatible recipient.
Virtual cross‑match is performed first and refers to the comparison, by the computer, of the HLA antibodies present in each candidate with the HLA antigens present in the kidney available. All candidates with specific antibodies against the loci A–, B‑ or DR‑ of the donors
HLA are immediately excluded. If the virtual cross‑match is negative, the candidates pursue the cytotoxic cross‑match, where the serum of each candidate is put together with lymphocytes of the donor. If the serum contains HLA donor specific antibodies capable of engaging a CDC response, the cells of the recipient become lysed and the candidate is excluded.
Although CDC‑PRA and cPRA are performed prior to transplantation (considering the pool of HLA phenotypes of the population) and virtual and cytotoxic cross‑matches are performed after a kidney donor is available (considering the specific HLA phenotype of the kidney to be donated), there is a relationship between them. In fact, cPRA reflects the probability of obtaining a positive virtual cross‑match and CDC‑PRA the probability of obtaining a positive CDC cross‑match.
Since to proceed in the selection process the candidate must first obtain a negative virtual cross‑match, the cPRA is a major determinant of the transplantability of each candidate reflecting (more accurately than CDC‑PRA) the candidates chance of receiving a kidney transplant2,4,5. The French and American entities responsible for organ allocation (Agence de la Biomedicine and OPTN/UNOS, respectively) therefore currently use cPRA as the measure of sensitization for awarding extra allocation points. This happened seven years ago, in 20096,7. In Portugal, the use of cPRA has already been proposed to become part of the kidney allocation algorithm2,5, but this has not yet happened.
Our aim was to determine candidates waiting time according to their cPRA and if the additional points offered to HS patients as defined by CDC‑PRA by the current allocation system are also benefiting HS patients as defined by cPRA.
SUBJECTS AND METHODS
Patients on the active list for kidney transplantation in Hospital de Santo António in 2014 were considered. Patients with no serum available were excluded. CDC‑PRA and cPRA were obtained for each patient. For cPRA, the most recent serum available was used.
Patients serum was screened to identify antibodies against various HLA class I and class II loci (HLA‑A, HLA‑B, HLA‑C and HLA‑DR, HLA‑DQ, HLA‑DP).
If the screening test was positive, the antibodies were identified using Single Antigen Beads Luminex technology. The periodic screening for antibodies against HLA is part of the protocol defined for maintenance of candidates on the active waiting list for kidney transplantation (specified in Regulatory Circular 01/DQS, of 7th January 2009, issued by the Directorate General of Health). In accordance with these rules, when determining cPRA only the anti‑HLA antibodies against – A, – B and – DR were considered. An antibody against HLA was considered positive if it had a mean fluorescence intensity (MFI) equal or superior to 1000. The frequency of HLA phenotypes of the population of the Northern part of Portugal was estimated from the frequency of bone marrow donors HLA phenotype, available in the database of the Centro do Sangue e Transplantaçãodo Porto.
Waiting time corresponds to time since dialysis was started, and was therefore calculated by subtracting the date of the first dialysis session from the date of sera collection.
STATISTICAL ANALYSIS
Continuous data were described using mean (standard deviation) or median (interquartile range) and categorical data were expressed as numbers (frequencies).
Categorical data were compared using Pearson χ2 test (χ2 for trend test was used when in the presence of a variable with 3 ordinal categories) or Fishers exact test, as appropriate. Continuous variables were compared with Student t‑test (or one‑way ANOVA for variables with 3 categories) or Mann‑Whitney U test (Kruskal‑Wallis test for variables with 3 categories), as appropriate. A Cohens Kappa analysis was performed to assess inter‑rater reliability between CDC‑PRA and cPRA.
A two‑sided P value <0.05 was considered as statistically significant. Statistical calculations were performed using SPSS for Mac, version 23.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
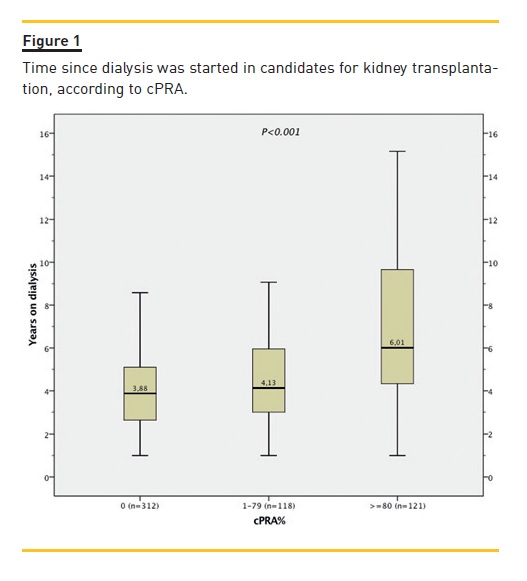
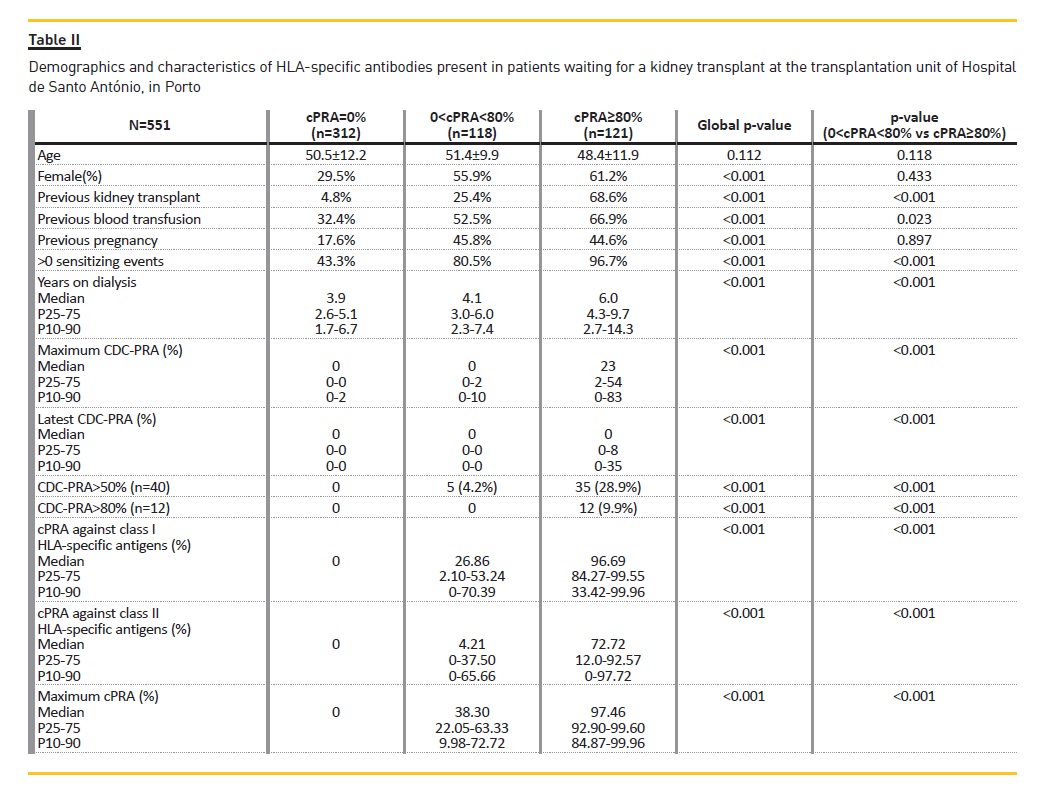
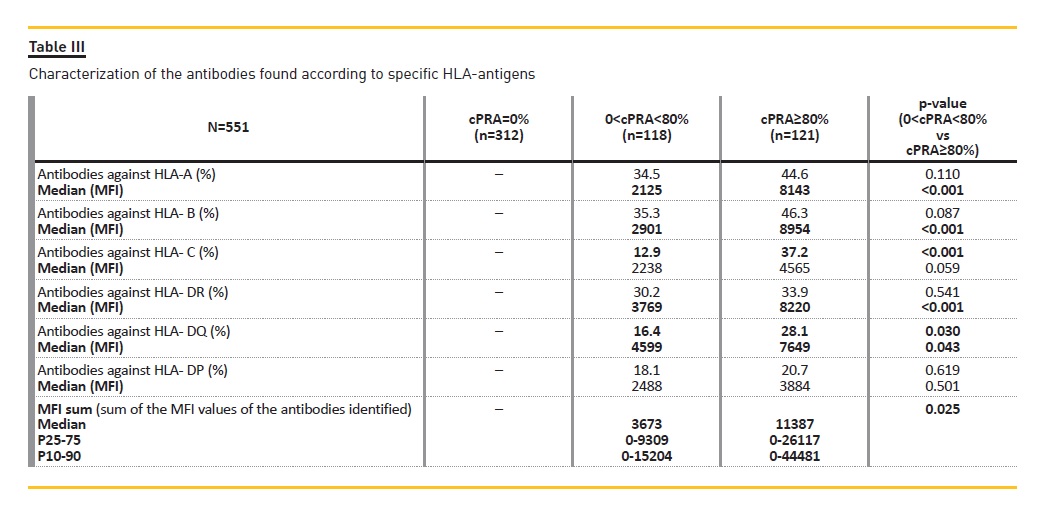
We included 551 patients and divided them into three groups (those with cPRA of 0%, those with cPRA between 1 and 79% and those with cPRA equal or superior to 80%). Female gender prevalence was higher in the cPRA>0% groups. Of the 551 patients included, 22% (N=121) had a cPRA ≥ 80%. HS patients included more women and more patients with previous sensitizing events (previous transplant, pregnancy or blood transfusion). Half of these patients –50.4% (n=61) – had been on the waiting list for more than 5 years; 31.4% (n=38) for more than 8 years and 18.2% (n=22) for more than 10 years. The median time on dialysis waiting for a transplant increased significantly with the cPRA (3.9 years in those with a cPRA of 0%; 4.1 years in those with a cPRA between 1 and 79% and 6.0 years in those with a cPRA equal or superior to 80%, P<0.001) (Fig. 1). Additional data regarding demographics, percentage of patients with prior sensitizing events, time on dialysis and values of CDC‑PRA and cPRA for HLA class I or II antigens are presented in Table II (both medians and percentiles are provided). The intensity of the antibodies found (in MFI units) and their characterization according to specific HLA antigen is described in Table III.
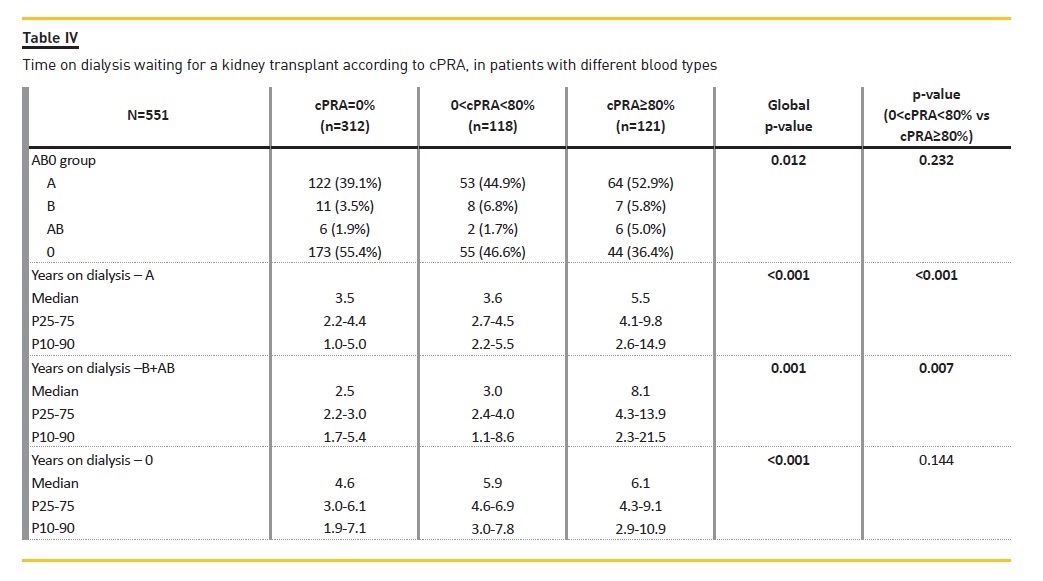
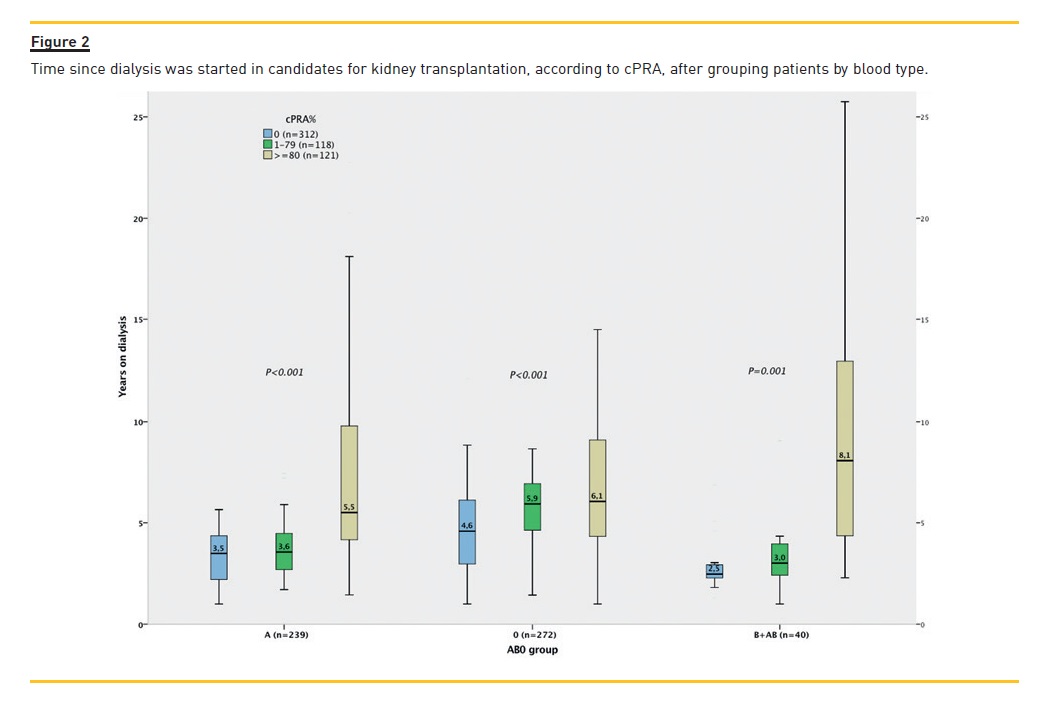
Since time waiting for a kidney transplant varies according to the candidates blood group, this was considered in a separate analysis (Table IV). The most frequent blood group of candidates for kidney transplant in our unit was group 0, followed by group A, B and AB. When comparing time on dialysis according to cPRA among patients grouped by blood type, waiting time continued to increase significantly with cPRA in all AB0 isogroups (Fig. 2).
The majority of the HS patients are relatively young. In fact, 82.6% (n=100) were aged less than 60 years old and 51.2% (n=62) aged less than 50 years old. Four HS candidates were children.
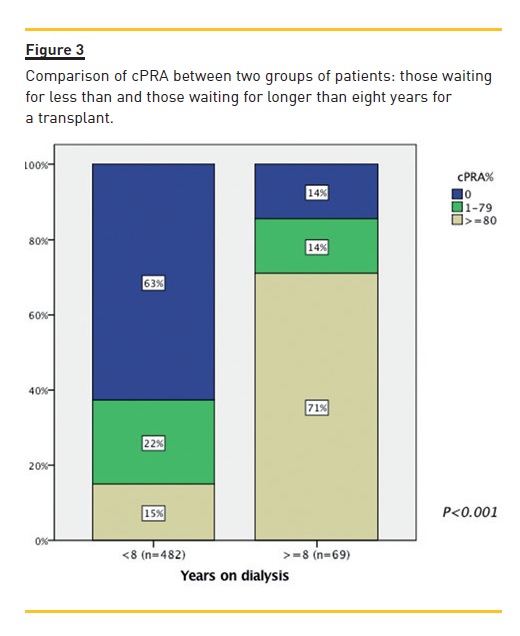
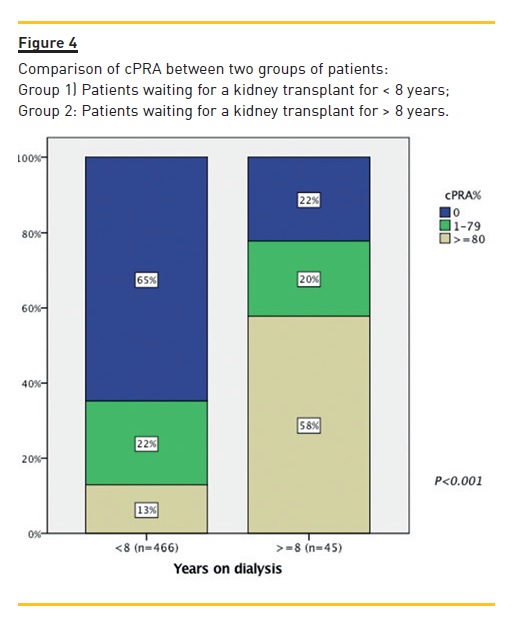
HS patients by cPRA corresponded to 71% vs 15% of patients waiting for more or less than 8 years, respectively (P<0.001) (Fig. 3). Even after exclusion of patients with a CDC‑PRA above 50%, this disproportionate representation remained (58% versus 13%, P<0.001) (Fig. 4).
In the group with a cPRA ≥ 80%, the median of the CDC‑PRA raised no suspicion of HS status (median CDC‑PRA of 0%, P25‑75 0‑8% – Table II). In fact, only 35/121 patients (28.9%) and 12/121 (9.9%) had a CDC‑PRA in the peak serum higher than 50 or 80%, respectively (50 and 80% correspond to the cut‑offs established by Portuguese law to receive 4 or 8 additional points in the kidney allocation algorithm – Ordinance nº 6537/2007 from April 3rd).
Cohens Kappa analysis showed low agreement between CDC‑PRA and cPRA when defining HS state (Table V). In fact, 71% of hypersensitized patients defined by cPRA> 80% have a CDC‑PRA < 50%, receiving no compensatory points during the allocation process.
DISCUSSION
Twenty‑two percent of the patients analyzed were found to have a cPRA equal or superior to 80%. This percentage is significant and is twice as high as that found in the United States in 2010 (11%)6. The reality of the French transplantation unit of Saint‑Louis seems more similar to ours, with 16.7 % of patients on the waiting list for kidney transplant in 2010 having a cPRA higher than 85%7.
Previous kidney transplant was shown to be a major sensitizing event, as has already been reported. C. Lechaufer et al., for example, found that of the 93 patients on the waiting list aiming for retransplantation, 82.8% were considered to be sensitized due to the presence of HLA specific antibodies7.
Our data demonstrate that HS patients as defined by cPRA wait longer for a kidney transplant. Bruno A. Lima et al.1 reported a median waiting time among all candidates for deceased‑donor kidney transplantation in the same transplant unit that we analyzed of 59.5 months (4.96 years). This paper considered patients transplanted between 2008 and 2011 (after the 2007 ordinance was issued, which established the current allocation policy). These findings are consistent with the ones now reported. The median waiting time of patients with cPRA ≥ 80% (6.0 years) was superior to the median previously reported, consolidating the hypothesis that these HS patients face an unfair disadvantage in accessing transplantation. Also, these results show that the current allocation system is not compensating for this disadvantage in an efficient manner.
Because these patients are held back in the selection process, they are then expected to be kept waiting for a transplant. This problem is therefore expected to aggravate, as HS candidates accumulate on the waiting list, further increasing the waiting time difference between those with low and high cPRA.
The chance that each candidate has of being transplanted must be stated clearly, if we aim for a transparent kidney allocation system2. Identifying patients with high cPRA may help the physician to inform patients about their real chance of being transplanted in the current allocation system (in France, for example, the theoretical number of compatible donors can be estimated to decide whether the sensitized patient has a donor flow considered to be sufficient or if undergoing a desensitization strategy would be more advantageous7).
That information can also be useful for patients in doubt as to whether to proceed with a living donation process. In the face of the transplantability of each individual patient, alternatives such as paired donor transplantation5 can also be discussed. These aspects gain importance if we consider that, according to our data, HS patients are relatively young (48 years on average).
Finally, time on dialysis while waiting for a kidney transplant is a crucial determinant of the success of the transplant itself1; hence the importance of making sure that patients access to transplantation is equal among all the candidates, and that the success of transplantation of HS patients is not jeopardized by an unfairly prolonged waiting time.
When analyzing waiting time in patients with different blood groups, our results were also consistent with those previously reported. Between 2008 and 2011 in Porto1, blood type A and 0 were the more frequently present, and AB the rarest. In that data series, blood type 0 candidates also waited longer than patients with other blood types for a kidney transplant. Although there was a change in the allocation policy in 2007 so that the recipient needs to be AB0‑identical to the donor (AB0 compatibility is not sufficient to proceed with transplantation), the heterogeneous waiting time according to blood type still persists.
In the analyzed cohort, patients had higher cPRA than CDC‑PRA. This was expected, as HLA‑specific antibodies that connect to the beads containing a specific HLA antigen may be present in amounts insufficient to engage a complement‑dependent cytotoxic response leading to cell lysis. Moreover, these results are consistent with those reported in the literature6. Also, in Portugal the CDC‑PRA identifies only cytotoxic antibodies against HLA‑A and HLA‑B (the assay employed does not identify antibodies specific for HLA‑DR, which are included when performing the virtual cross‑match).
This may help explain why patients have higher cPRA (that also takes into consideration antibodies against HLA‑DR) than CDC‑PRA.
However, the opposite is also possible, with previous studies reporting cases of patients with CDC‑PRA higher than the cPRA3. The main reason for this is the presence of IgM antibodies in the candidate. In other countries, the discrepancy between CDC and calculated PRA may be also due to the presence of DP or DQ HLA antibodies not identified by the cytotoxic assay. Since in Portugal only antibodies against HLA‑A, HLA‑B and HLA‑DR are considered in the virtual cross‑match, only these were considered in our study to calculate the cPRA.
Despite all the additional information provided by the cPRA, the authors consider that the cPRA should be viewed as a complement (not as a replacement) of the CDC‑PRA, and the virtual cross‑match should be considered as the first step evaluation, with a cytotoxic cross‑match performed routinely thereafter5.
Patients with high CDC‑PRA are less likely to find a compatible kidney. As such, previous studies have already demonstrated that they wait longer for a transplant. Since a considerable amount of those with high CDC‑PRA also have high cPRA, it could be argued that CDC‑PRA could be responsible for the increased waiting time among the HS defined by the cPRA. However, our results show that, even after excluding patients with CDC‑PRA> 50%, cPRA ≥ 80% continues to be associated with an increased waiting time.
Therefore, patients with cPRA ≥ 80% and a CDC‑PRA< 50% also wait longer but do not receive compensatory points in the allocation algorithm. This issue affects a significant amount of HS patients, since the majority (70%) of patients with cPRA ≥ 80% do not receive additional points during allocation (see Cohen Kappa analysis in Table V showing low agreement between CDC‑PRA and cPRA).
Of the 475 transplants performed in Porto between 2008 and 2011, only 1.5% of the recipients had a peak CDC‑PRA ≥ 50%1. Conversely, in the United States between 2001 and 2002, 7.3% of the total of kidney transplants were performed in HS (CDC‑PRA ≥ 80%) patients4.
Other allocation systems struggle with the difficulty in providing HS patients equal access to kidney transplantation.
In the United States, for example, although the virtual cross‑match is performed early in the recipients selection process, it is the transplant centres responsibility to decide the threshold of intensity of anti‑HLA antibodies (measured in MFI) above which the virtual cross‑match is considered positive and the candidate is excluded6. This cut‑off must not be set too low (in HS candidates many HLA antigens would be considered unacceptable, preventing them from proceeding to the cytotoxic cross match that might turn out to be negative) nor too high (so that the efficiency of allocation is not compromised by the need to perform an exceedingly large number of CDC cross‑matches that will most definitely turn out to be positive6).
Instead, the transplant centre needs to balance individually the risk and benefit of each candidate receiving an allocated kidney, taking into account the possibility of undertaking a desensitization therapy, as well as the probability of getting an alternative donor against which the recipient could have an improved HLA‑compatibility.
However, the current Portuguese system does not allow each transplant unit to consider different MFI thresholds to define unacceptable antigens adapted to the candidates immunological complexity when performing the virtual cross‑match (any antibody with intensity higher than 1000 MFI, either in the last or in any of the historical sera, is considered unacceptable). Therefore, the majority of these HS patients are immediately excluded in the virtual cross‑match, so that many of them will never receive additional points. Proof that the compensation points are ineffective is the fact that despite the current legislation, HS patients continue to wait significantly longer for a kidney transplant. In other words, these patients long waiting times places them high on the candidates list only to immediately exclude them in the virtual cross‑match.
It could be feared that a legislation change could reverse the situation by providing HS patients with preferential access to transplantation, creating a new injustice. Since the allocation policy in the United States started to consider cPRA to define HS status, the percentage of transplants performed in HS patients increased to 15.8% in 2009‑2010.
HS and nonsensitized patients transplant rates became closer without giving any unfair advantage in transplantation access to any of these two groups6.
As established by Ordinance nº 6537/2007, Ordinance nº 11420/2008 and further specified in the Regulatory Circular Nº 15/GDG of 7 September 2009, transplantation should only be considered in the absence of known previous allosensitization against specific antigens present in the donor. A positive virtual cross‑match reflects the presence of allosensitization against the donor. Therefore, these candidates are immediately excluded, even though they might not have a positive cytotoxic cross‑match.
Moreover, if the candidate has had a positive donor specific antibody in any of the previously collected sera, he/she cannot proceed with transplantation. Although previous sera results should be considered in evaluating immunological risk and when planning desensitization strategies, we consider that only the antibodies against the donor present in the most recent serum should be taken into account in the decision on whether the candidate should proceed to a cytotoxic cross‑match.
Also, since Ordinance nº 11420/2008 was published, the kidney selection for hypersensitized patients is no longer performed at a national level, but only at a regional level. By lowering the available pool of donors for these patients, the chance HS patients have of finding a compatible kidney has been further reduced.
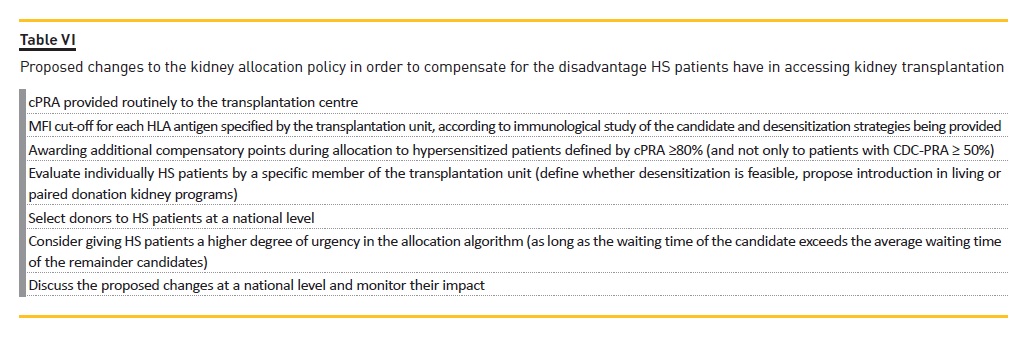
In conclusion, several aspects could be improved in order to compensate for the disadvantage HS patients have in accessing transplantation (Table VI). The authors consider that the identification of patients with high cPRA is important and that cPRA should be shared routinely with the transplantation centre. Also, the allocation system could be improved if cPRA was taken into consideration (by setting an individualized MFI cut‑off on the virtual cross‑match in the face of the antibody type and its relationship to the cytotoxic assays and by giving additional compensatory points to all patients with high PRA – either cPRA or CDC‑PRA).
Moreover, the authors consider that these patients benefit from an individualized evaluation by a specific member of the transplantation unit, including design of appropriate desensitization strategies in the face of the donor flow for the HLA phenotype of the candidate, inclusion in the paired kidney donation programme, or a combination of both. Finally, selecting donors for HS patients at a national (not regional) level and attributing HS patients undergoing desensitization a higher degree of urgency in the allocation algorithm should be considered (as long as the waiting time of the candidate exceeds the average waiting time of the remainder candidates). All these proposals should be discussed nationally, in order to obtain consensus between the different transplantation units.
References
1. Lima BA, Mendes M, Alves H. Kidney Transplant allocation in Portugal. Port J Nephrol Hypert. 2013; 27(1): p. 313‑316. [ Links ]
2. Lima BA, Mendes M, Alves H. Kidney Transplant Allocation in Portugal. Port J Nephrol Hypert. 2013; 27(4): p. 1‑4. [ Links ]
3. Ji‑Young J, Yoon‑Joo K, Yoonggoo K, Yeon‑Joon P, Kyungia H, Eun‑Jee O. Application of Calculated Panel Reactive Antibody Using HLA Frequencies in Koreans. Ann Lab Med. 2012; 32: p. 66‑72. [ Links ]
4. Cecka JM, Kucheryavayab AY, Reinsmoenc NL, Leffell MS. Calculated PRA: Initial Results Show Benefits for Sensitized Patients and a Reduction in Positive Crossmatches. Am J Transplant. 2011; 11: p. 719‑724. [ Links ]
5. Lima BA, Mendes M, Alves H. Hypersensitized candidates to kidney transplantation in Portugal. Port J Nephrol Hypert. 2013; 27(2): p. 77‑81. [ Links ]
6. Leffell MS. The calculated panel reactive antibody policy: an advancement improving organ allocation. Curr Opin Organ Transplant. 2011; 16(4): p. 404‑409. [ Links ]
7. Lefaucheur C, Antoine C, Suberbielle C, Glotz D. Mastering the Risk of HLA Antibodies in Kidney Transplantation: An Algorithm Based on Pretransplant Single‑Antigen Flow Bead Techniques. Am J Transplant. 2011; 11: p. 1592‑1598. [ Links ]
Rita Aires Magriço
Rua Luís Pastor de Macedo, Lote 17/18 3º D
E‑mail: rita.magrico@yahoo.com
Disclosure of Conflicts of Interest: None declared.
Received for publication: Nov 9, 2015
Accepted in revised form: Apr 28, 2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}