










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.29 no.4 Lisboa dez. 2015
CASE REPORT
Idiopathic nodular glomerulosclerosis: a case report
Glomerulosclerose nodular idiopática: caso clínico
Catia Cunha1, Ana Marta Gomes1, Daniela Lopes1, Sonia Sousa1, Susana Pereira1, Sofia Campelos2, David Tente2, Joao Carlos Fernandes1
Centro Hospitalar de Vila-Nova de Gaia/Espinho, Vila -Nova de Gaia, Portugal.
1 Department of Nephrology.
2 Department of Pathology.
ABSTRACT
The histological pattern of nodular glomerulosclerosis is typical of diabetic nephropathy, but it can be found in other diseases, such as chronic membranoproliferative glomerulonephritis, amyloidosis, monoclonal immunoglobulin deposition and fibrillary/immunotactoid glomerulopathies. Additionally, there are few reports of idiopathic nodular glomerulosclerosis, an exclusion diagnosis, which has been associated with smoking. Herein we present a case of a non-diabetic 45-year-old man, with a background history of hypertension known for 5 years and heavy smoking, who was referred to our Nephrology clinic for evaluation of haematoproteinuria.
Renal function was normal and serologies and immunoelectrophoresis studies were negative. Renal biopsy revealed a nodular glomerulosclerosis pattern on light microscopy, and immunofluorescence and electronic microscopy excluded other previously referred causes for this pattern. By exclusion, a diagnosis of idiopathicnodular glomerulosclerosis was established, probably in association with smoking and hypertension. Idiopathic nodular glomerulosclerosis is a distinct clinicopathologic entity that should be considered in patients with active smoking, especially if there is concomitant hypertension. Some authors actually suggest the designation of smoking -related nodular glomerulosclerosis to this pseudodiabetic glomerulopathy.
Key -Words: Hypertension; nodular glomerulosclerosis; smoking.
RESUMO
O padrão histológico de glomeruloesclerose nodular é típico da nefropatia diabética, mas pode ser encontrado noutras patologias como na glomerulonefrite membranoproliferativa crónica, na amiloidose, nas glomerulopatias associadas a deposição de imunoglobulinas e nas glomerulopatias fibrilar e imunotactóide. Adicionalmente, há alguns casos descritos de glomeruloesclerose nodular idiopática, um diagnóstico de exclusão, que tem sido associado ao tabagismo. Apresentamos o caso de um doente de sexo de masculino, 45 anos de idade, não diabético, com antecedentes de hipertensão arterial diagnosticada há 5 anos e fumador pesado, que foi referenciado à nossa consulta de Nefrologia por hematoproteinúria. Estudo revelou função renal normal e estudo imunológico e imunoelectroforese foram negativas. Biópsia renal revelou um padrão de glomeruloesclerose nodular na microscopia de luz e a imunofluorescência e microscopia electrónica excluíram as outras causas previamente referidas para este padrão. Por exclusão, foi estabelecido o diagnóstico de glomeruloesclerose nodular idiopática, provavelmente em associação com o tabagismo e hipertensão. Glomeruloesclerose nodular idiopática é uma entidade clinicopatológica distinta que deve ser considerada em doentes fumadores activos, particularmente na presença concomitante de hipertensão. Alguns autores sugerem mesmo a designação de glomeruloesclerose nodular associada ao tabagismo a esta glomerulopatia pseudodiabética.
Palavras-Chave: Glomeruloesclerose nodular; hipertensão; tabagismo.
INTRODUCTION
The histological pattern of nodular glomerulosclerosis, previously considered pathognomonic of diabetic nephropathy (DN), is now known to be present in several other entities. Idiopathic nodular glomerulosclerosis (ING) is one of these entities and the term was first introduced, in 1999, by Herzenberg et al. to describe patients who had nodular glomerulosclerosis without evidence of diabetes or other specific diseases1. Despite initially considered idiopathic, it has been increasingly described in the last decade as associated with smoking and hypertension.
Tobacco use constitutes a major public health problem, which leads to increased morbidity and mortality. Carcinogenesis effects, cardiovascular and lung disease associated with smoking are well established.
The effects in the kidney are not so evident, but it is known that smoking is related to microalbuminuria in healthy people and may impair renal function by several mechanisms2.
An independent clinical entity, ING is histologically similar to DN, which can be attributed to heavy smoking. Its role as a cause of glomerular disease is highlighted in the patient herein described with diagnosis of nodular glomerulosclerosis.
CASE REPORT
We present a case of a 45-year-old Caucasian man who was referred to our nephrology clinic because of microscopic haematuria and proteinuria. He had a background of hypertension diagnosed 5 years before, for which he was medicated with olmesartan 20 mg per day at diagnosis, achieving a good control of his blood pressure. His medical history included additionally dyslipidaemia (on atorvastatin 10 mg daily), active smoking (22 pack -years), an estimated alcohol consumption of 60 to 70 g per day and a body mass index of 27 kg/m2. No history of diabetes was reported and the family history was irrelevant.
On the first visit he was completely asymptomatic. Physical examination revealed a blood pressure of 140/82 mmHg, unremarkable heart and lung examinations and no peripheral oedema.
Pertinent laboratory results included a normal serum creatinine of 0.7 mg/dL (normal range 0.67-1.17 mg/dL), a normal full blood count, normal serum albumin, high total cholesterol of 275 mg/dL (normal range < 200 mg/dL), high LDL of 173 mg/dL (normal range 3 -100 mg/dL) and an elevation of gama glutamil transferase (1.5 times the upper limits of normal), but normal transaminases and alkaline phosphatase. Serum fasting glucose was normal at serial evaluations and glycosylated haemoglobin was 5% (normal range 3.9 -6.2%). Urinalysis showed microscopic haematuria and the urine protein-creatinine ratio was 2.44. Immunological screening was normal (including immunoglobulin levels, complement C3 and C4, antinuclear antibody, anti-dsDNA and ANCA) and serologies for HCV, HBV and HIV were negative. No monoclonal immunoglobulins were detected on serum and urinary electroimmunofixation. No abnormalities were found on renal ultrasound.
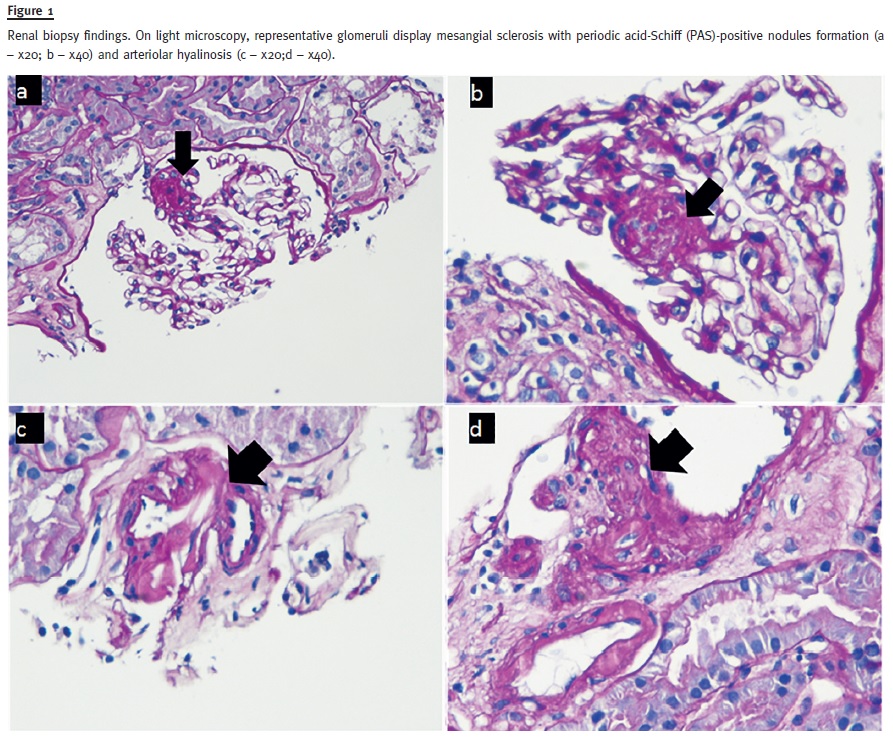
On renal biopsy (Fig. 1), light microscopy showed eleven glomeruli: two with a nodular glomerulosclerosis pattern, two with global glomerulosclerosis, one with segmental glomerulosclerosis, one with ischaemic changes and five with no abnormalities. Arteriolar hyalinosis was also present. There was no glomerular basement membrane thickening or duplication and no crescents or fibrinoid necrosis were found. Mild interstitial fibrosis and tubular atrophy occupied less than 5% of the cortex. Congo red staining was negative.
Immunofluorescence revealed 2+ intensity granular segmental focal capillary and tubular basement membrane positivity for C3; and 1+ intensity for C4 and C1q with the same distribution. On electron microscopy, the podocyte foot processes were focally effaced, there was also a mesangial and capillary membrane sclerosis and rare subendothelial deposits were found on mesangio -capilar transition; no fibrils were detected.
A diagnosis of ING was established, probably in association with smoking and hypertension. Angiotensin II blocker was maintained and the patient was advised to stop smoking.
One year after renal biopsy, there was still no evidence of diabetes mellitus. Blood pressure was controlled on monotherapy with olmesartan 20 mg daily. The patient managed to cut down but did not quit smoking, and agreed to be referred to the smoking cessation clinic. His creatinine at one-year follow-up was 0.95 mg/dl and urine protein-creatinine ratio 1.46.
DISCUSSION
The histological pattern of nodular glomerulosclerosis is a very well known pattern seen in DN, also called Kimmelstiel-Wilson nodules3. However, the differential diagnosis is vast and includes chronic membranoproliferative glomerulonephritis; dysproteinemias as amyloidosis and monoclonal immunoglobulin deposition; organized glomerular deposition diseases, such as fibrillary, immunotactoid, fibronectin and collagen III glomerulopathies; and chronic hypoxic or ischaemic conditions, such as Takayasus arteritis with renal artery stenosis, cyanotic congenital heart disease and cystic fibrosis4,5. These entities usually are readily distinguished by integration of clinical history and serologies with fluorescence microscopy and electron microscopic findings on renal biopsy6. Our patient had no diabetes and the clinical evaluation, laboratory results and biopsy excluded all the previous diagnosis. By definition, ING is an exclusion diagnosis and has been described in association with smoking and chronic hypertension, which is consistent with our clinical case.
Idiopathic nodular glomerulosclerosis is now considered a distinct clinicopathological entity characterized by nodular glomerulosclerosis in patients without a subjacent disease. It is a rare diagnosis.
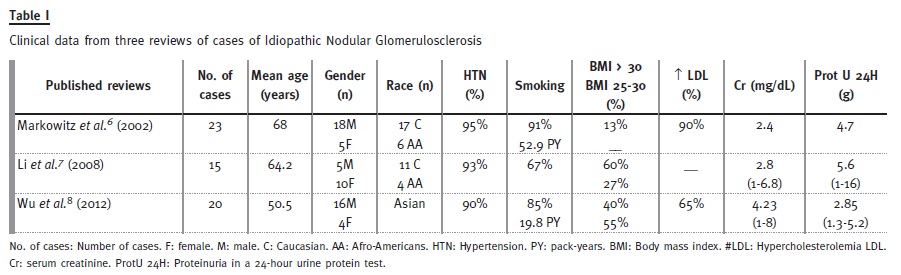
In the literature, we found three recent reviews which included a total of only 58 patients6-8 (relevant data presented in Table I), but other isolated clinical cases have been published9-16. Two of the reviews included Caucasian and Asian patients6,7, while one included exclusively Asian patients8. The average age at presentation varied from 50.5 to 68 years in these studies. Markovitz et al. 6 and Wu et al. 8 found an increased prevalence of males, but in the study by Li et al. 7 two thirds of the affected patients were females. Taking into consideration all cases published in Pubmed (72 cases), male gender seems to be predominant, corresponding to 64% of cases8.
The gender distribution requires additional clarification.
Almost all patients described were hypertensive (90 -95%) and in the great majority were smokers, in spite of variable percentages (67 -91%). One study showed that most were heavy smokers with a mean cumulative intake of 52.9 pack -years, while in another study the average was much less, 19.2 pack -years6,8.
Most patients were overweight or obese, except in the study by Markovitz et al., where obesity was present in only 13% of cases (no data for overweight is available)6-8. Dislipidemia, defined as an increased LDL, was also prevalent, present in 90% of cases in the study by Markowitz et al. and 65% in the Chinese study by Wu et al. 6,8. Race and biases due to small sampling might explain the differences between these studies.
Globally, ING seems to target especially hypertensive mid-age male smokers, with obesity and dyslipidemia as potential contributing factors. Our male patient has also hypertension, smoking habits, dyslipidemia and overweight. He was, however, younger than the average, but ING has been previously described in younger patients. The youngest patient was a 13-year-old African American girl and the oldest an 80-year-old Caucasian woman11.
Regarding clinical presentation, most of the patients presented with proteinuria in the nephrotic range (average 2.85 – 5.6 g per day) and decreased glomerular filtration rate, with an average serum creatinine of 2.4, 2.8 (1 -6.8) and 4.23 (1 -8) mg/dL in the different studies6-8.
The findings in renal biopsies include diffuse and nodular mesangial sclerosis, which justifies its name, but also thickening of glomerular basement membrane (GBM), and arteriosclerosis6,7. Some have additional features of DN, such as Bowmans capsular hyalinosis, glomerular microaneurisms, tubular basement membrane thickening and afferent and efferent arteriolar hyalinosis6. The nodules are Periodic Acid Shift positive (PAS +), show reactivity with silver stain and have no affinity for Congo red dye5. Immunofluorescence microscopy may show non-specific linear staining of GBM and tubular basement membrane for IgG and albumin in about half of the cases and focal segmental coarsely granular tuft staining for IgM and C3 in areas of sclerosis is displayed in most cases, but immune deposits are not present5-7.
GBM thickening and foot process effacement is visible by electron microscopy, which should also exclude the presence of immune electron-dense deposits or fibrils5-8.
The mechanisms behind the association between smoking and ING are still under investigation. One of the potential mechanisms is the formation of advanced glycation end products (AGE), known to accumulate in the mesangial nodules and zones of interstitial fibrosis in both ING and DN4. Smoking also exerts effects on intrarenal haemodynamics, mainly through sympathetic activation, which induces renal vasoconstriction and, consequent, reductions in renal blood flow and glomerular filtration rate17. Increased angiogenesis also seems to be an important factor. Both the direct effect of nicotine and the indirect effect of hypoxia in smokers who develop chronic obstructive pulmonary disease may play a role in stimulating angiogenesis4.
Finally, smoking promotes oxidative injury to the endothelium, which is suggested by the mild features of thrombotic microangiopathy present in some cases of ING6.
Despite the suggested role of smoking in the aetiology of ING, the scarcity of this diagnosis suggests that additional environmental factors, comorbidities and/or genetic susceptibility may interact to result in the disease8. Smoking-induced renal damage occurs preferentially in the setting of pre-existing sclerotic insult, which in ING seems to be hypertensive nephrosclerosis4. So, ING can representa special form of hypertensive arterionephrosclerosis that is modified by smoking4.
Markovitz et al.6 showed a median time from biopsies to end-stage renal disease (ESRD) of only 26 months. Severity of interstitial fibrosis/tubular atrophy and arteriosclerosis were predictors of progression to ESRD, but that was not, however, confirmed in another study8. Different population characteristics and more severe renal dysfunction on presentation in the latter could have explained the discrepancy.
Regarding the treatment, Markovitz et al. demonstrated that cessation of smoking and angiotensin II blockers administration improve renal survival6.
The median renal survival in smokers was 11 months, whereas none of the patients who had discontinued smoking reached ESRD during a mean follow-up of 14.2 months6. However, regression of these lesions was never unequivocally demonstrated. The role of inhibition of the renin-angiotensin system in preventing the progression of chronic glomerular injury in diabetic and non-diabetic patients was proved in many clinical trials. The benefits may be related to the ability of these agents to prevent the overproduction of mesangial matrix induced by glomerular hypertension or the production of transforming-growth factor-beta13. Weight loss in obese patients, use of antioxidants and other anti-inflammatory treatments may be also beneficial in addressing the progressive inflammatory response associated with ING7.
CONCLUSION
Idiopathic nodular glomerulosclerosis is a distinct clinicopathological entity that should be considered in patients with active smoking, especially if there is concomitant hypertension. Some authors actually suggest the designation of smoking-related nodular glomerulosclerosis to this pseudodiabetic glomerulopathy, as the term idiopathic seems to have become obsolete as the underlying aetiology emerges.
References
1. Herzenberg AM, Holden JK, Singh S, Magil AB. Idiopathic nodular glomerulosclerosis. Am J Kidney Dis 1999; 34(3):560 -564. [ Links ]
2. Orth SR, Ogata H, Ritz E. Smoking and kidney. Nephrol Dial Transplant 2000; 15(10):1509 -1511. [ Links ]
3. Kimmelstiel P, Wilson C. Intracapillary lesions in the glomeruli of the kidney. Am J Pathol 1936; 12(1):83 -98.7. [ Links ]
4. Nasr SH, DAgati VD. Nodular glomerulosclerosis in the nondiabetic smoker. J Am Soc Nephrol 2007; 18(7): 2032 -2036. [ Links ]
5. Raparia K, Usman I, Kanwar YS. Renal morphologic lesions reminiscent of diabetic nephropathy. Arch Pathol Lab Med 2013; 137(3): 351 -359. [ Links ]
6. Markowitz GS, Lin J, Valeri AM, Avila C, Nasr SH, DAgati VD. Idiopathic nodular glomerulosclerosis is a distinct clinicopathologic entity linked to hypertension and smoking. Human Pathol 2002; 33(8): 826 -835. [ Links ]
7. Li W, Verani RR. Idiopathic nodular glomerulosclerosis: a clinicopathologic study of 15 cases. Human Pathol 2008; 39(12): 1771 -1776. [ Links ]
8. Wu J, Yu S, Tejwani V, et al. Idiopathic nodular glomerulosclerosis in Chinese patients: a clinicopathologic study of 20 cases. Clin Exp Nephrol 2014; 18(6): 865 -875. [ Links ]
9. Kasmani R, Thiyagarajan T, Narwal -Chadha R, Okoli K, Irani F. The other end of spectrum in hypertension: Idiopathic nodular glomerulosclerosis. Int Urol Nephrol 2010; 42(3): 857 -859. [ Links ]
10. Müller-Höcker L, Weiss M, Thoenes GH, Grund A, Nerlich A. A case of idiopathic nodular glomerulosclerosis mimicking diabetic glomerulosclerosis (Kimelstiel–Wilson type). Pathol Res Pract 2002;198(5): 375 -379. [ Links ]
11. Kuppachi S, Idris N, Chander PN, Yoo J. Idiopathic nodular glomerulosclerosis in a non-diabetic hypertensive smoker – case report and review of literature. Nephrol Dial Transplant 2006; 21(12): 3571-3575. [ Links ]
12. Liang KV, Greene EL, Oei LS, Lewin M, Lager D, Sethi S. Nodular glomerulosclerosis: Renal lesions in chronic smokers mimic chronic thrombotic microangiopathy and hypertensive lesions. Am J kidney disease 2007; 49(4): 552 -559. [ Links ]
13. Kusaba T, Hatta T, Sonomura K, et al. Idiopathic nodular glomerulosclerosis: three Japanese cases and review of the literature. Clin Nephrol 2007; 67(1): 32 -37. [ Links ]
14. Halmai R, Degrell P, Szijártó IA, et al. Smoking as the potencial link between Kimelstiel-Wilson lesion and non-diabetic nodular glomerulosclerosis in male patients – a single center retrospective study. Clin Nephrol 2013; 80(1): 23 -28. [ Links ]
15. Costa AF, Gomes dos Santos WA, Gonçalves MA, Modesto dos Santos V. Nodular glomerulosclerosis in a non -diabetic hypertensive smoker with dyslipidemia. An Sist Sanit Navar 2011; 34(2): 301 -308. [ Links ]
16. Kinoshita C, Inoue Y, Kanda Y, Kanda C. A case of idiopathic nodular glomerulosclerosis with fibrin caps. Clin Exp Nephrol 2011; 15(6): 937 -941. [ Links ]
17. Grassi G, Seravalle G, Calhoun DA, et al. Mechanisms responsible for sympathetic activation by cigarette smoking in humans. Circulation 1994; 90(1): 248 -253. [ Links ]
Drª Cátia Cunha
Department of Nephrology,
Centro Hospitalar de Vila -Nova de Gaia/ Espinho
Rua Conceição Fernandes, 4434 -502 Vila Nova de Gaia, Portugal.
E-mail: catiatcunha@gmail.com
Conflict of interest statement: None declared.
Received for publication: 03/08/2015
Accepted in revised form: 21/10/2015


{kind=link}
{kind=link}