










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.28 no.2 Lisboa jun. 2014
CASE REPORT
Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman
Rubina Naqvi1, Muhammed Mubarak2
1Department of Nephrology
2Department of Histopathology Sindh Institute of Urology and Transplantation (SIUT). Karachi, Pakistan.
ABSTRACT
Dual positive cases of anti-glomerular basement membrane (GBM) antibody and anti-neutrophil cytoplasmic antibody (ANCA) associated nephritis are not rare in clinical nephrology practice. These patients often present with a clinical picture of rapidly progressive GN (RPGN). Published studies indicate that up to 30% of patients with anti-GBM antibody nephritis have associated ANCA antibodies in their sera. On the other hand, only up to 5% of ANCA-associated GN patients have anti-GBM antibodies. There are conflicting reports in the literature on the significance of double positive antibodies on the presentation, clinical course and outcome of these patients. It is possible that the predominant behaviour depends on the predominance or time of appearance of either antibody. However, all studies conclude that the recovery of renal functions is rare with dual positivity of the above antibodies. We herein present a case of a middle-aged lady presenting with non-specific features of renal failure and was diagnosed to have crescentic GN on renal biopsy and both anti-GBM and ANCA antibodies in the serum. We discuss the management of this case in the light of existing literature on this subject.Key words: Anti-GBM antibody; ANCA; Crescentic glomerulonephritis; rapidly progressive glomerulonephritis; serology; renal failure.
INTRODUCTION
Dual positive cases of anti-glomerular basement membrane (GBM) antibody and anti-neutrophil cytoplasmic antibody (ANCA) associated nephritis are not uncommon. These patients often present with a clinical picture of rapidly progressive GN (RPGN) or acute renal failure (ARF)1-5. Typically, anti-GBM antibody nephritis presents acutely and is associated with a monophasic picture on histology, with all the crescents on renal biopsy exhibiting similar stage of evolution. The recurrence rate is also low. Studies show that up to 30% of patients with anti-GBM antibody nephritis have associated ANCA antibodies in their blood3-5. On the contrary, 5% of ANCAassociated GN patients have anti-GBM antibodies in their sera2,3. There are conflicting reports in the literature on the significance of double positive antibodies on the presentation, clinical course and outcome of the patients6-10. A few studies have shown that patients with dual positive antibodies have a poor prognosis when presenting with severe disease and behave more like anti-GBM disease rather than as vasculitis3. Other investigators have suggested that these cases behave more like vasculitis4. It is presumed that the predominant behaviour depends on the predominance or time of appearance of either antibody5-7. However, all authors agree that the recovery of renal functions is rare with dual positivity of the above antibodies11-13. We have earlier presented a case with the clinical presentation of RPGN followed by respiratory failure in an elderly woman5.
Briefly, she was a 65-year-old woman presenting with advanced uremic symptoms and serum creatinine of 21.3 mg/dl. She had both anti-GBM and ANCA antibodies positive in her serum. Interestingly, the ANCAs were of both pANCA and cANCA types, a phenomenon very rarely reported in the literature.
Her biopsy showed predominantly cellular crescents, but there were some fibrocellular and fibrous crescents.
Moderate degree of tubular atrophy was also seen. She was started on dialysis, plasmapharesis and intense immunosuppression, but despite above measures developed diffuse alveolar haemorrhage and died of respiratory failure.
We herein present a case of a middle-aged lady presenting with non-specific features of renal failure and diagnosed to have crescentic GN and both anti-GBM and ANCA antibodies in the serum. We discuss the management of this case in the light of existing literature on this subject.
CASE REPORT
A 45-year-old female with no past history of note, was admitted to some other hospital with generalized weakness and decreased appetite of 4 weeks.
She gave a vague history of nausea and occasional vomiting over the last 8 months. She also complained of passing less urine and at presentation had a urine volume less than 250 ml/day. She was referred to this institution for abnormal renal functions. In the past medical history, she had hypothyroidism and was on thyroxine replacement therapy for the last 12 years, with recent thyroid stimulating hormone (TSH) level of 15.4 uIU/ml (Normal range: 0.34 to 5.60 uIU/ml). Family history was unsuggestive.
On general physical examination at arrival, she was stable vitally, with blood pressure of 120/80 mm of Hg. General and systemic examination revealed no abnormality except for 2+ oedema on dependent parts.
Initial laboratory results were as: haemoglobin, 11.5 g/dl; total leukocyte count (TLC), 21.8×109/l; platelets, 184×109/l; blood urea nitrogen, 187 mg/dl; creatinine, 14.15 mg/dl; sodium, 125 mEq/L; potassium, 2.2 mEq/l; chloride, 86 mEq/l; bicarbonate, 17 mEq/l; calcium, 9.2 mg/dl; phosphorus, 9.4 mg/dl; albumin, 2.4 g/dl; and alkaline phosphatase, 59 U/l. Urinalysis revealed: albumin, 3+; red blood cells (RBCs), numerous; and white blood cells (WBCs), numerous.
Serology revealed: C3- 1.01 g/l; C4- 0.39 g/l; antinuclear antibody (ANA), weak positive (1:40); antidsDNA, negative; hepatitis B and C, negative; antiglomerular basement membrane (GBM), strong positive (78.13 U); p-ANCA, positive with anti-myeloperoxidase (MPO), > 100 U.
Chest roentgenogram was unremarkable. Abdominal sonography was unremarkable except for multiple, non-obstructing gall stones. Both kidneys were of normal size.
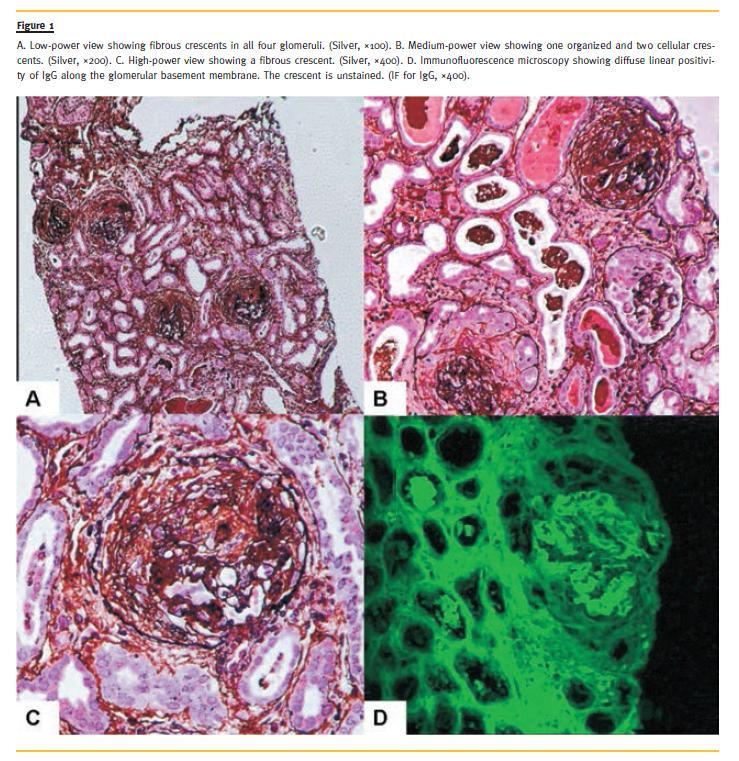
Renal biopsy done on the third day of admission comprised of cortex only with up to 12 glomeruli. All of these were grossly abnormal with 10 showing fibrous crescents and 2 fibrocellular crescents (Fig. 1 A, Fig. 1 B, Fig. 1 C). No arteritis was found. There was moderate to severe degree of tubular atrophy associated with interstitial scarring and inflammation. Immunofluorescence (IF) showed diffuse, linear positivity of IgG, while rest of the renal panel was negative (Fig. 1 D).
She was started on haemodialysis on the second day of admission and was treated with 3 doses of pulse steroids (750 mg/day), followed by oral prednisolone (1 mg/kg/day). After the availability of results of renal biopsy on the fourth day of admission, she was administered pulse cyclophosphamide (750 mg intravenously) and daily plasmapheresis in standard doses, according to the body weight, for 12 sessions. She remains dialysis dependent until the last followup, which is 4 months from first presentation. Oral steroids were tapered down and stopped over the next 4 months.
DISCUSSION
The serologic evidence of double positivity for both ANCA and anti-GBM antibodies is fairly common in patients with either antibody-associated renal pathology and a clinical picture of RPGN or ARF1-5.
Up to 30% of patients with anti-GBM antibody nephritis have associated ANCA positivity1,6,7. In the majority of cases, the ANCAs have been reported to belong to pANCA variety. On the other hand, the prevalence of anti-GBM antibodies is low in patients with ANCA-associated GN, usually reported to be positive in around 5% of cases1,8. We have earlier reported a case of doubly positive antibodies-associated RPGN that had both types of ANCA antibodies in addition to anti-GBM antibodies, a phenomenon very rarely reported in the literature5. The current case, however, had only p-ANCA positivity in association with anti-GBM antibodies. The previous case also developed severe pulmonary involvement during the course of illness and the disease proved fatal.
In contrast, we were able to salvage the current patient, however, she did not recover renal function.
Moreover, the present case also did not develop lung pathology as in the previous case. There are very few case reports in the literature with this presentation9,14.
One case reported by Neary et al.9, had cANCA positivity in association with anti-GBM antibody. No triggering or inciting factor was identified in our present case.
The published literature on this subject shows that patients with dual positive antibodies have a poor prognosis when presenting with severe disease and behave more like anti-GBM disease than vasculitis1,3,11-13. The present case also behaved like anti-GBM disease rather than vasculitis. The disease occurred in a young adult female with no constitutional symptoms. The biopsy pathology was predominantly monophasic, had diffuse linear positivity of IgG along GBM and the titer of anti-GBM antibodies was markedly high. It is highly likely that the admixture of some active glomerular lesions may reflect damage of these structures by the ANCA antibodies, on a background of chronic changes induced by anti-GBM antibodies. Other investigators have suggested that these patients behave as vasculitisvariant of anti-GBM antibody nephritis4. Presumably, the predominant behaviour depends on the predominance and the time of appearance of either antibody.
The recovery of renal functions is, however, rare with dual positivity of the above markers.
The management of anti-GBM antibody-associated disease involves three main steps: removal of the antibody from the circulation by plasmapharesis; prevention of further antibody production by immunosuppressant therapy; and eliminating or avoiding repeated exposure to potential triggering agents1,4,10-13.
However, the key to successful management is the early diagnosis and prompt institution of therapy.
Delay in these procedures often leads to fatal outcome as in our previous case5. Although renal histology in the present case was suggestive of chronic process of some duration, we treated the patient with intense immunosuppression and plasmapharesis to rescue renal function and to forestall pulmonary complications.
We were able to rescue the patient but, unfortunately, her renal failure did not improve. This outcome is essentially in agreement with the latest Kidney Disease Improving Global Outcomes (KDIGO) guidelines on the management and prognosis of this disease15.
According to these guidelines, patients who are dialysis-dependent at the start of treatment and have 85-100% glomerular crescents, do not recover renal function, despite intense immunosuppression.
Thus, in hindsight, it appears that we over-treated the patient and the treatment was also started late.
In fact, the patient also presented to us late in the first place. These factors led to the lack of recovery of renal functions despite intense immunosuppression.
The patient is on regular dialysis and waiting for renal transplantation. Her anti-GBM antibody titers have become undetectable 2 months after presentation.
There is very little evidence regarding the appropriate time of transplantation in such patients. Most transplant centres require at least 6 months of undetectable anti-GBM antibody titers before undertaking transplant procedure. Recurrence of the disease with this approach is very rare15.
In summary, we have presented a case with double positive serology for anti-GBM antibodies and ANCAs and a clinical picture of RPGN in a middle aged lady without pulmonary complications. A prompt diagnosis and treatment is essential to salvage the kidney and the patient.
References:
1. Javed T, Vohra P. Crescentic glomerulonephritis with anti-GBM and p-ANCA antibodies. Case Rep Nephrol 2012;132085. [ Links ]
2. Zhao J, Yang R, Cui Z, Chen M, Zhao MH, Wang HY. Characteristics and outcome of Chinese patients with both antineutrophil cytoplasmic antibody and antiglomerular basement membrane antibodies. Nephron Clin Pract 2007;107(2):c56-c62. [ Links ]
3. Hijosa MM, Roman LE, Camblor CF, Garcia ML, Salcedo DP, Torres MN. Anti-GBM and anti-MPO antibodies coexist in a case of pulmonary renal syndrome. Pediatr Nephrol 2005;20(6):807-810. [ Links ]
4. Levy JB, Hammad T, Coulthart A, Dougan T, Pusey CD. Clinical features and outcome of patients with both ANCA and anti-GBM antibodies. Kidney Int 2004;66(4):1535-1540. [ Links ]
5. Naqvi R, Mubarak M. Rapidly progressive renal failure followed by respiratory failure in an elderly woman. J Nephropathol (in press). [ Links ]
6. Rutgers A, Heeringa P, Damoiseaux JG, Tervaert JW. ANCA and anti-GBM antibodies in diagnosis and follow-up of vasculitic disease. Eur J Int Med 2003;14(5):287-295. [ Links ]
7. Yang G, Tang Z, Chen Y, et al. Antineutrophil cytoplasmic antibodies (ANCA) in Chinese patients with anti-GBM crescentic glomerulonephritis. Clin Nephrol 2005;63(6):423-428. [ Links ]
8. Serratrice J, Chiche L, Dussol B, et al. Sequential development of perinuclear ANCAassociated vasculitis and anti-glomerular basement membrane glomerulonephritis. Am J Kidney Dis 2004;43(3):e26-e30. [ Links ]
9. Neary P, Kadlubowski M, Thomson D, Cavaye M, Cumming AD. Antiglomerular basement membrane disease with cANCA positivity without pulmonary involvement. Nephrol Dial Transplant 1996;11(4):693-695. [ Links ]
10. Lindic J, Vizjak A, Ferluga D, et al. Clinical outcome of patients with coexistent antineutrophil cytoplasmic antibodies and antibodies against glomerular basement membrane. Ther Apher Dial. 2009;13(4):278-281. [ Links ]
11. DE Zoysa J, Taylor D, Thein H, Yehia M. Incidence and features of dual anti-GBMpositive and ANCA-positive patients. Nephrology (Carlton). 2011;16(8):725-729. [ Links ]
12. Rutgers A, Slot M, van Paassen P, van Breda Vriesman P, Heeringa P, Tervaert JW. Coexistence of anti-glomerular basement membrane antibodies and myeloperoxidase-ANCAs in crescentic glomerulonephritis. Am J Kidney Dis 2005;46(2):253-262. [ Links ]
13. Murakami T, Nagai K, Matsuura M, et al. MPO-ANCA-positive anti-glomerular basement membrane antibody disease successfully treated by plasma exchange and immunosuppressive therapy. Ren Fail 2011;33(6):626-631. [ Links ]
14. Yang R, Hellmark T, Zhao J, et al. Antigen and epitope specificity of anti-glomerular basement membrane antibodies in patients with goodpasture disease with or without anti-neutrophil cytoplasmic antibodies. J Am Soc Nephrol 2007;18(4):1338-1343. [ Links ]
15. Chapter 14: Anti-glomerular basement membrane antibody . Kidney Inter 2012; Suppl 2; 240-242.
Prof. Dr. Rubina Naqvi
Department of Nephrology, Sindh Institute of Urology and Transplantation
Karachi-74200, Pakistan,
Email: rubinanaqvi@gmail.com
Conflict of interest statement: None declared.
Received for publication: 09/10/2013
Accepted in revised form: 25/02/2014


{kind=link}