










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.28 no.2 Lisboa jun. 2014
REVIEW ARTICLE
Relationship of Vitamin D with Diabetes Mellitus and Diabetic Nephropathy
Relação entre a Vitamina D com a Diabetes Mellitus e a Nefropatia Diabética
Ana Paula Silva, Andre Fragoso, Pedro Leao Neves
Department of Nephrology, Hospital de Faro – Centro Hospitalar do Algarve. Faro, Portugal
ABSTRACT
Diabetic nephropathy (DN) is a major public health problem whose prevalence has been increasing in recent years. It is characterized by a progressive pattern and is associated with high morbidity and mortality rates. Several factors are associated with the onset and progression of DN, such as glycaemic control, hypertension, obesity and inflammation status. In addition, vitamin D also seems to be involved through a pleiotropic regulatory activity/protection with promising applicability, either in prevention or progression of renal disease. The purpose of this review was to summarize the scientific evidence that supports the role of vitamin D in diabetes mellitus and DN.
Key-Words: Diabetes mellitus; diabetic nephropathy; vitamin D.
RESUMO
A nefropatia diabética (ND) e um problema de saúde pública grave, cuja prevalencia tem vindo a aumentar nos últimos anos. A ND e caracterizada por um padrão de progressão e está associada a taxas de morbilidade e mortalidade elevadas. Diversos fatores são associados com o surgimento e progressao da ND, tais como o controle glicemico, a hipertensão, a obesidade e o estado inflamatório. Além disso, a vitamina D parece também estar envolvida, através de uma actividade reguladora pleiotropica/protectora com uma aplicabilidade promissora, tanto na prevenção como na progressão da doença renal. O objectivo deste artigo de revisão e sumarizar a evidência cientifica que suporta o papel da vitamina D na diabetes mellitus e na ND.
Palavras-Chave: Diabetes mellitus; nefropatia diabetica; vitamina D.
INTRODUCTION
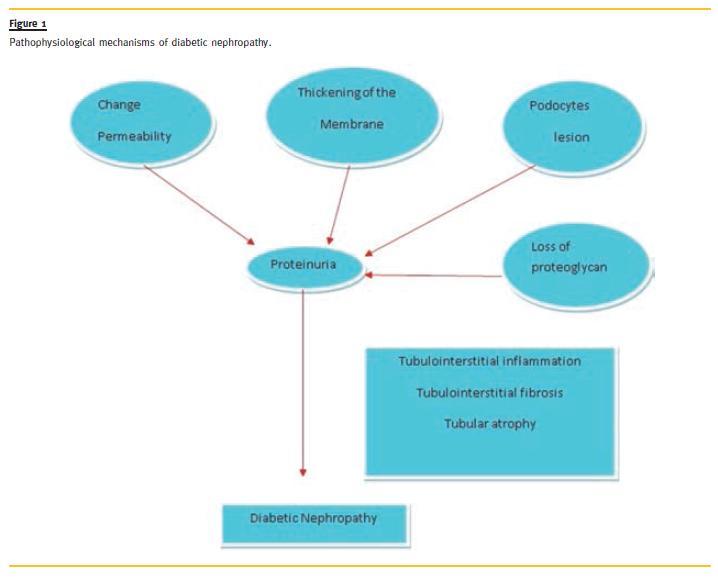
Proteinuria is a classic marker of glomerular impairment and it has been implicated as a key factor for the progression of kidney disease1.
Diabetic nephropathy (DN) is clinically characterized by the onset of proteinuria and its progression to chronic renal disease is currently the leading cause of end-stage renal failure requiring renal replacement techniques in industrialized countries2,3. In addition to its increasing incidence, DN is associated with a high rate of cardiovascular mortality, whose risk is two to three times higher when associated with proteinuria4. The metabolic changes induced by diabetes mellitus (DM) are per se sufficient for the development of the glomerular lesions observed in DN. There are several retrospective and prospective studies that confirm it, particularly the Diabetes Control and Complications Trial (DCCT), and the United Kingdom Prospective Study (UKDPS), with type 1 and type 2 diabetic patients, respectively. These studies have demonstrated that the development of DN is influenced by metabolic control. However, some diabetic patients with good metabolic control developed DN, while others preserved a normal renal function and did not present proteinuria, despite a poorer glycaemic control. These observations suggest that in diabetes, hyperglycaemia is an important but not sufficient factor to cause renal lesions5. Although hyperglycaemia is the major determinant in the pathogenesis and progression of DN, this pathologic process can be modified by genetic susceptibility and accelerated by several other factors6. (Fig. 1)
Regarding vitamin D (1,25 dihydroxivitamin D3, the active form of Vitamin D3), and supported by the presence of its receptors in several organs and tissues, it is known that it has a role in other processes and pathways besides the activity on mineral metabolism7-9. Adequate levels of 1,25 dihydroxivitamin D3 are important for maintaining the good functioning of bone metabolism, and there is also evidence of its anti -proliferative effect in cellular differentiation, immunomodulation and inhibition of the renin-angiotensin system (RAS)10.
There is evidence that in kidney disease, podocytes are affected in glomerular disease and that they play an important role in the progression to more advanced stages, including nephropathy in type 1 and type 2 diabetes11.
Recently, some experimental studies have documented the existence of 1,25 dihydroxivitamin D3 receptors (VDR) in podocytes and have demonstrated an association between this vitamin and the number of podocytes observed. This association may contribute to the prevention and reduction of mesangial cells proliferation and to promote a decrease in proteinuria12.
Supporting this evidence, Schwarz et al. demonstrated that treatment with 1,25 dihydroxivitamin D3 attenuates the development of glomerulosclerosis and the progression of albuminuria in rats submitted to subtotal nephrectomy13. Other studies also demonstrated that the administration of 1,25 dihydroxivitamin D3 reduces mesangial cells proliferation, glomerular hypertrophy and progression to glomerulosclerosis14 -16. The 1,25 dihydroxivitamin D3 has a pleiotropic effect, which indicates a regulatory/protective role with promising applicability, either for preventing or treating chronic kidney disease17-19.
The objective of this article was to summarize the scientific evidence regarding the role of 1,25 dihydroxivitamin D3 in DM and DN.
VITAMIN D
The 1,25 dihydroxivitamin D3 and its receptors have a role in the transcription of several genes responsible for the activation or inhibition of many proteins, thereby playing an important role in the pathophysiology of certain diseases6,20.
1,25 dihydroxivitamin D3 receptor
The 1,25 dihydroxivitamin D3 is an important modifier of gene transcription, even in tissues that are not involved in calcium homoeostasis, and acts by regulating the synthesis of messenger RNA (mRNA).
This biological action is triggered after binding to VDR, with predominantly nuclear localization6. This receptor forms a complex with the Retinoid-X–receptor (RXR), resulting in a heterodimer complex with VDR that migrates into the cell nucleus and interacts with the 1,25 dihydroxivitamin D3 response element (VDRE) in the DNA, leading to the transcription, or not, of genes implicated in several biological functions21.
Plasma membrane -associated VDR (mVDR) is responsible for the rapid responses of 1,25 dihydroxivitamin D3, associated with its non-genomic action. The biochemical structure of these receptors is not yet known but their action is achieved through the opening of calcium or chlorine channels and mitosis activator proteins22,23.
Genomic and non- genomic action of Vitamin D
The 1,25 dihydroxivitamin D3 has a dynamic and configurationally flexible structure that allows multiple physiological responses on target tissues through the activation of genomic and non-genomic mechanisms22,23. Through the nuclear VDR, it causes activation or inhibition of the expression of genes responsible for the transcription of specific proteins.
This process may occur for hours or days and it is recognized as its genomic response24.
Nuclear VDR is a ligand dependent transcription factor, modulating the expression of genes 1,25 dihydroxivitamin D3 dependent, via three mechanisms25:
–Upregulation of the expression of certain genes by allowing binding to VDRE present in the DNA promoter region (osteocalcin, osteopontin, Nuclear Factor -KappaB [NF -Kb] activator receptor);
– Downregulation of the expression of other genes, by not allowing binding to VDRE;
– Inhibition of the expression of some genes through the antagonistic action of specific transcription factors, which are the nuclear factors, namely the nuclear factor of activated T-cells (NFAT) and NF-KB26,27.
The genomic mode of action of this active form involves a direct interaction of VDR with the DNA sequence, with 200 genes being regulated by this hormone, however, little is known about the mechanisms involved28. On the other hand, it can also act through an alternative receptor, mVDR, which stimulates the rapid formation of second messengers, protein kinases and the opening of calcium and chlorine channels, triggering a variety of cellular responses within seconds or minutes. This process is recognized as a non -genomic response to 1,25 dihydroxivitamin D325-28. Therefore, this hormone may have a key role in the prevention and treatment of some diseases, including type 1 and type 2 diabetes, as well as in microvascular (nephropathy, retinopathy and diabetic neuropathy) and macrovascular (coronary artery disease, cerebrovascular and peripheral arterial disease) complications28.
VITAMIN D AND DIABETES MELLITUS
Diabetes mellitus is associated with microvascular and macrovascular complications. Some observational studies have reported the association between 1.25 dihydroxivitamin D3 receptors and type 1 and type 2 DM, glucose intolerance, sensitivity to insulin secretion and serum calcitriol levels29-38.
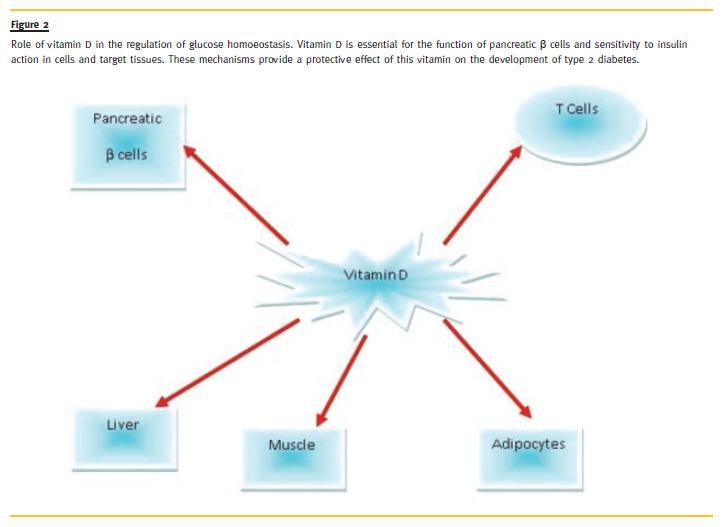
The pathophysiology of type 2 diabetes is complex, but we know that there is an involvement of changes in pancreatic β-cell function and tissue resistance to insulin. It is generally accepted that as the major hormone regulating calcium metabolism, 1,25 dihydroxivitamin D3 produces effects on the immune system and on the pancreatic β cells by facilitating insulin production38 (Fig. 2).
The presence of 1,25 -dihydroxyvitamin D3 receptors in the pancreas raises the possibility of a direct action of this vitamin in the synthesis, regulation and secretion of pancreatic hormones. It was recently reported the presence of 1,25 dihydroxivitamin D3 -dependent-calcium -binding protein (DBP) in the pancreatic β cells and an additional factor in favour of the action of this vitamin in regulating the synthesis and secretion of insulin verified that 25-hydroxyvitamin D is converted to its active form, 1.25–dihydroxyvitamin D, in the pancreatic β cells through the action of the 25 -hydroxyvitamin D -1α -hydroxylase39-40.
Hypovitaminosis D is a risk factor for the development of type 2 diabetes and metabolic syndrome since it causes pancreatic β cell dysfunction and peripheral resistance to insulin action41. Supplementation in patients with type 2 diabetes and non-diabetic patients with hypovitaminosis enhances the secretion of insulin, suggesting that this vitamin improves the action of the islets of Langerhans β cells42.
The mechanism by which 1,25 dihydroxivitamin D3 deficiency contributes to the onset of type 2 diabetes is not fully understood, and more studies are necessary to further examine this association; however, it is clear that pancreatic β cell dysfunction, resistance to insulin action and low -grade inflammation are important factors for the development of glucose intolerance and type 2 diabetes42-44.
In both animal and human studies, it was described that pancreatic β cell dysfunction is associated with a state of 1,25 dihydroxivitamin D3 deficiency and that its supplementation contributes to the conversion of pro -insulin into insulin45. Despite the evidence of a protective role of this vitamin in diabetes, it is unclear whether its deficiency is related to the several risk factors presented in this disease46-47.
VITAMIN D AND DIABETIC NEPHROPATHY
The mechanisms associated with DN are multiple and complex, being all interconnected, and this process is not yet fully understood.
Role of cellular and molecular mediators in diabetic glomerulopathy
The key determinant factor for the pathogenesis and progression of DN is hyperglycaemia, and this process can be modified by genetic susceptibility or accelerated by other factors, such as hypertension, proteinuria, hypercholesterolaemia, and smoking habits, among others48.
The glomerulus is the location of histological lesions associated with DM, where mesangial cell proliferation, the excessive production of extracellular matrix (fibronectin, laminin, collagen type IV), occurs due to increased levels of intracellular glucose.
This high glucose concentration induces the overexpression of glucose transporter (GLUT -1) mRNA, triggering production of the GLUT1 protein in mesangial cells, which leads to an increased urinary excretion of transforming growth factor β1 (TGF-β1)49-51. This factor has an important role on the onset and progression of DN, by inducing the production and accumulation of fibronectin and collagen IV in the extracellular matrix resulting in structural changes in the glomerulus (interstitial fibrosis and sclerosis)52-54.
The mechanisms associated with DN are not fully understood, and many of the molecular factors associated with the renal lesion are under investigation.
However, it is known that there are four mechanisms responsible for the onset of DM complications that are triggered by the increase of intracellular glucose.
These mechanisms are:
– Increased flow through the polios pathway, with consequent increase of sorbitol in the tissues, including the renal tubules and glomeruli. This increase in sorbitol causes tissue lesion by changing the cellular osmoregulation. This is the primary mediator of protein kinase C (PKC) cellular activation55;
– The increase in the non-enzymatic advanced glycosylation end products (AGEs) causes an increase in plasma proteins and extracellular matrix. When AGEs bind to specific receptors, identified in the macrophages of endothelial and mesangial cells, they induce the synthesis and secretion of cytokines (IL TNF -α, IL -1, IL -6) and insulin growth factor (IGF1), stimulating mesangial cells proliferation and collagen IV production. Moreover, by crosslinking with collagen, AGEs can induce an increase in extracellular matrix synthesis by stimulating growth factors (TGF -β1, CTGF, VEGF, PDGF)56;
– Increase of the flow through the hexosamine pathway, causing changes in gene expression of glomerular cells and endothelial cells55.
These mechanisms are, among others, responsible for the changes in the glomerular filtration barrier whose manifestation is the emergence of proteinuria.
Role of the renin -angiotensin- aldosterone system (RAAS):
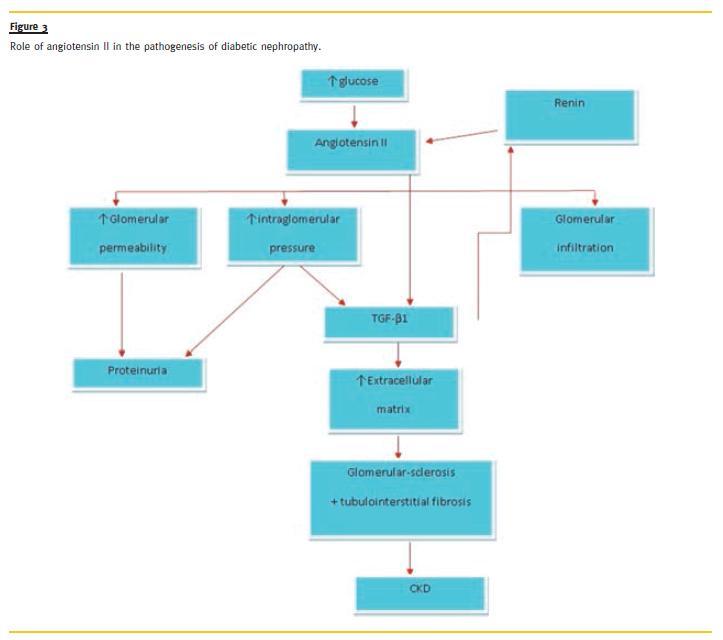
Hyperglycaemia stimulates the production of cytokines, including the angiotensin II (Ang II). This is a vasoactive peptide with glomerular hemodynamic actions that contributes to the onset of proteinuria (Fig. 3).
Angiotensin II has a pro-fibrotic, pro–angiogenic and pro -inflammatory actions. It is the main mediator of TGF β1 and connective tissue growth factor (CTGF) production at the level of mesangial and tubular cells, leading to an increased production of extracellular matrix and contributing to the development and progression of glomerulosclerosis and tubulointerstitial fibrosis, typical features of DN57. It regulates mesangial cell growth, by promoting glomerular proliferation or hypertrophy, and also promotes an increased expression and synthesis of extracellular matrix proteins, such as fibronectin, laminin, and collagen IV58.
In its pro -angiogenic action, hypoxia triggers increased expression and synthesis of VEGF, contributing to the progression of renal lesion59.
Currently, the role of Ang II in slit diaphragm of podocytes is under investigation, especially on the integrity of components (nephrin, podocin and α-actin – 43) and haemodynamic mechanisms responsible for proteinuria60,61. Angiotensin II and growth factors interfere with the haemodynamic mechanisms and structural/metabolic manifestations of the DN.
Cellular changes of podocytes and diabetic nephropathy
The onset of proteinuria in diabetic patients is a sign of changes in the glomerular filtration barrier, which consists of endothelium, basement membrane and podocytes. The function of this barrier is to limit the passage of macromolecules, primarily according to size, electrical charges (molecules with negative charges have more difficulty in crossing) and shape of the molecule itself62. Podocytes are responsible for maintaining the structure and functioning of the barrier.
These are highly differentiated cells and their lesion causes dysfunction of the barrier with immediate consequences in the pathogenesis of proteinuria11.
Podocytes also express a number of proteins, which contribute to this high degree of differentiation, some of which are specific of these cells. These proteins, localized in the podal processes, are responsible for maintaining cell shape and function. Some seem to be involved in the pathophysiology of proteinuria by modulating the function of the subpodocytic slit diaphragm. Some studies revealed that haemodynamic mechanisms modulate the changes of podocytes specific proteins, including nephrin, with a decrease of its expression and consequently an increased urinary excretion of proteins63. Histomorphometric studies in animal models of type 1 diabetes with proteinuria, showed an apparent fusion of podocytes, which assume a flattened shape with disappearance of the space between the podal processes64.
This morphological change triggers a breakdown of the subpodocytic slit diaphragm, with the podocytes losing much of their ability to contain the passage of macromolecules, causing urinary excretion of increased amounts of proteins, as long as the lesion persists. However, an analysis of renal biopsies during the European Study for the Prevention of Renal Disease Type 1 Diabetes (ESPRIT), in normotensive patients with albuminuria, showed no significant reduction in the number of podocytes as compared to the non-diabetic control group65. However, longitudinal studies have demonstrated a clear correlation between the reduction in the number of podocytes during follow-up and proteinuria66,67.
In renal biopsies performed in Pima Indians with type 2 diabetes, it was found not only a deletion but also a reduction in the number of podocytes68.
Schiffer et al, demonstrated that hyperglycemia alters the expression of regulatory proteins and induces apoptosis in renal tubular and endothelial cells. There is also evidence that TGF -β1 plays an important role in the pathogenesis of DN and causes apoptosis in podocytes in culture69.
Vitamin D mechanisms of action in DN
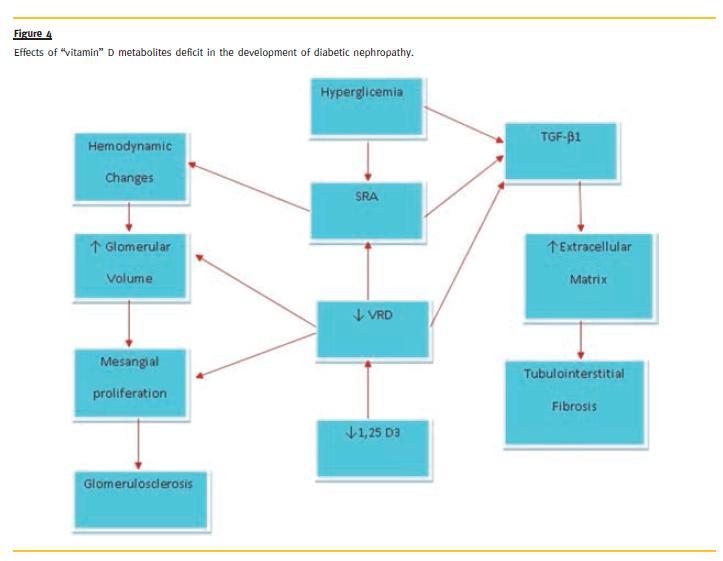
Hyperglycaemia causes the intrarenal production of factors by downregulating VDR and 1α-hydroxylase in proximal tubule cells, resulting in a decreased tubular megalin expression and consequently a decrease in 1,25 dihydroxivitamin D3 reabsorption with increased levels of protein urinary excretion70.
The combination of hyperglicaemia and the absence of VDR results in an intrarenal increase of RAAS activation, as demonstrated by Zhang, and simultaneously there is evidence that deficits in the active metabolite of 125 dihydroxivitamin D3 indirectly stimulate the activation of TGF -1β71 (Fig. 4).
The mechanisms of action of 1,25 dihydroxivitamin D3 in the pathogenesis of proteinuria include haemodynamic and non-haemodynamic direct actions that regulate cell proliferation, apoptosis, angiogenesis and anti-inflammatory action. The 1,25-dihydroxyvitamin D3 seems to inhibit myofibroblasts proliferation in the renal interstitium by stimulating hepatocyte growth factors, thus performing a renoprotective effect by suppressing the activation of myofibroblasts production in the matrix72 -76.
In some experimental models, administration of 1,25 -dihydroxyvitamin D3 decreased the loss of podocytes and inhibited their hypertrophy77-79. This beneficial effect is due to a direct action in signal modulation, by inhibiting TGF -b1 and bone morphogenetic protein (BMP -7) expression80. In DN, the protective action of 1,25 dihydroxivitamin D3 is also due to its negative regulatory effect on the RAAS, by suppressing the production of renin which is one of the mechanisms responsible for renal injury, either by haemodynamic mechanisms, or through pro-inflammatory and pro--fibrotic mechanisms81-83. Although the mechanisms are not completely understood, 1,25 dihydroxivitamin D3 and its analogues, have protective functions by promoting the reduction of proteinuria, a biomarker of kidney involvement84,85.
Randomized Clinical trials of Active Vitamin D therapy in Proteinuria Several small studies have demonstrated the benefit of using 1,25 dihydroxivitamin D3 in reducing the levels of proteinuria in renal disease.
Agarwal and colleagues evaluated the efficacy of oral paricalcitol in 220 patients with stages 3 and 4 chronic kidney disease over a period of 24 months. In addition to other parameters, proteinuria was measured by dipstick at the start and at the end of the trial period84.
The 107 patients were randomized in a double-blind pilot trial, with 57 patients receiving oral paricalcitol. At the end of the study, patients treated with paricalcitol showed a greater reduction of proteinuria, 51 vs. 25.5 % in the placebo group (OR = 3.2 for reduction of proteinuria, 95% CI:1.5 -6.99). The effect of paricalcitol in reducing proteinuria was independent of demographic characteristics, comorbidities and use of antagonists of the renin -angiotensin system. The effect of paricalcitol in reduction proteinuria was independent of demographic characteristics, comorbidities and use of antagonists of the renin-angiotensin system84.
Also in a study with non -diabetic chronic kidney patients, Alborzi et al. showed the advantage of paricalcitol over placebo. In a shorter trial, these authors found that paricalcitol (1 and 2μg / day) reduced albuminuria in about 50%, comparing with placebo (p > 0.001)79. Oral calcitriol also reduced the proteinuria in a small group of patients with biopsy proven IgA nephropathy86. More recently, Aperis et al. also found, in a non-randomized study, that paricalcitol decreased albuminuria, in a heterogeneous group including diabetic and non-diabetic patients87.
Regarding diabetic patients, there are two clinical studies that only included type 2 diabetic patients.
In both, all patients were already medicated with antagonists of the renin-angiotensin system. The VITAL study was a prospective, randomized, double-blinded placebo-controlled, multicentre study that evaluated the efficacy of oral paricalcitol on reducing albuminuria:creatinine ratio (UACR). In this trial, 281 patients were equally allocated into 3 groups to receive, 0, 1 or 2 μg of oral paricalcitol for a 24-week period. Patients on 2 μg showed a statistically significant reduction in UACR of 20% (p = 0.014 vs. placebo)88.
In a prospective observational study, Kim et al. treated, with oral cholecalciferol, during four months, type 2 diabetic patients with low levels of 25(OH) D. They found that cholecalciferol reduced albuminuria and urinary TGF -β1 and concluded that dietary 1,25 dihydroxivitamin D3 repletion with cholecalciferol could have a beneficial effect on progression of DN89.
Despite the existence of several studies reporting the ability of 1,25 -dihydroxyvitamin D3 to lower proteinuria/albuminuria in diabetic and non-diabetic patients, quite a few questions remain unanswered.
First of all, it is crucial to look at hard end-points, like the progression of kidney disease, conducting studies with longer follow-up time. It is known that in PRIMO study, the administration of paricalcitol was associated with a greater decrease of the renal function90. Although this study was not designed to address the progression of the renal disease and the paricalcitol group had worst renal function at baseline, this study reinforced the need of an answer to this issue. Secondly, cardiovascular is the main cause of morbidity and mortality in chronic kidney patients and there is a bulk of evidence showing that low levels of 1,25 dihydroxivitamin D3 are associated with greater risk of cardiovascular events in the general population90-92. It will be very important to ascertain if the treatment of chronic kidney disease patients with 1,25 dihydroxivitamin D3 will decrease cardiovascular morbidity and mortality in this particular population.
In an observational study including diabetic and non -diabetic patients, we could find that patients undergoing treatment with statins in association with 1,25 dihydroxivitamin D3 (alfacalcidol) had lower mortality93. It would be also important to see if the results are the same by administrating 1,25 dihydroxivitamin D3 or paricalcitol, an activator of the 1,25 dihydroxivitamin D3 receptor, since in terms of costs it is quite different.
The knowledge of the right moment of intervention, with former normalization of the 1,25 dihydroxivitamin D3 levels, also seems crucial. Will it be useful to administrate paricalcitol in 1,25 dihydroxivitamin D3 repleted patients?
The inclusion of type 1 diabetic patients and the evaluation of cardiovascular end -points are fundamental in future trials, in order to investigate the benefits of 1,25 dihydroxivitamin D3 in chronic kidney disease patients with DN.
CONCLUSION
Through the activation of its nuclear receptors and consequent transcription of 200 genes, 1,25 dihydroxivitamin D3, leads to the activation or inhibition of several proteins. Due to these mechanisms of action, this vitamin may have a key role in the prevention and treatment of some diseases, including type 1 and type 2 diabetes, as well as in its complications, namely in DN.
However, many questions remain and must be answered by conducting longer trials with stronger renal and cardiovascular end-points.
References
1. Tabaei BP, Al -Kassab A, Zawacki CM, Herman WH. Does microalbuminuria predict diabetic nephropathy? Diabetes Care 2001;24(9):15160 - 15166. [ Links ]
2. Raptis AE, Viberti G. Pathogenesis of diabetic nephropathy. Exp Clin Endocrinol Diabetes 2001; 109 Suppl 2:S424 - 437. [ Links ]
3. Tervaert TW, Mooyaart AL, Amann K, et al. the Renal Pathology Society. Pathologic classification of diabetic nephropathy. J Am Soc Nephrol 2010; 21(4):556 -5 63. [ Links ]
4. Thomas SM, VibertiI GC. Cardiovascular risk in diabetic kidney disease: A model of chronic renal disease. Kidney Int 2005; 98 Suppl:S18 - S20. [ Links ]
5. McDonnell DP, Mangelsdorf DJ, Pike JW, Haussler MR, O`Malley BW. Molecular cloning of complementary DNA encoding the avian receptor for vitamin D. Science 1987; 235(4793):1214 - 1217. [ Links ]
6. Haussler MR, Haussler CA, Jurutka PW, et al. The vitamin D hormone and its nuclear receptor: molecular actions and disease states. J Endocrinol 1997; 154 Suppl:S57 -S73. [ Links ]
7. Holick MF. McCollum Award lecture, 1994: vitamin D -new horizons for the 21st century. Am J Clin Nutr 1994; 60(4):619 - 630. [ Links ]
8. Holick MF. Vitamin D: the underappreciated D -lightful hormone that is important for skeletal and cellular health. Curr Opin Endocrinol Diabetes 2002; 9(1):87 -98. [ Links ]
9. Holick MF. Vitamin D: A millenium perspective. J Cell Biochem 2003; 88(2):296 -307. [ Links ]
10. DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr 2004; 80(Suppl 6):1689S - 1696S. [ Links ]
11. Mundel P, Shankland SJ. Podocyte biology and response to injury. J Am Soc Nephrol 2002; 13(12):3005 - 3015. [ Links ]
12. Kriz W, Lemley KY. The role of the podocyte in glomerulosclerosis. Curr Opin Nephrol Hypertens 1999; 8(4):489-497. [ Links ]
13. Schwarz U, Amann K, Orth SR, Simonaviciene A, Wessels S, Ritz E. Effect of 1,25 (OH)2 vitamin D3 on glomerulosclerosis in subtotally nephrectomized rats. Kidney Int 1998; 53(6):1696 - 1705. [ Links ]
14. Weinreich T, Merke J, Schonermark M, et al. Actions of 1,25 -dihydroxyvitamin D3 on human mesangial cells. Am J Kidney Dis. 1991; 18(3):359 - 366. [ Links ]
15. Panichi V, Migliori M, Taccola D, et al. Effects of 1,25(OH)2D3 in experimental mesangial proliferative nephritis in rats. Kidney Int 2001; 60(1):87 - 95. [ Links ]
16. Vieth R. Vitamin D supplementation, 25 -hydroxyvitamin D concentrations, and safety. Am J Clin Nutr 1999; 69(5):842 - 856. [ Links ]
17. Grant WB, Holick MF. Benefits and requirements of vitamin D for optimal health: a review. Altern Med Rev 2005; 10(2):94 - 111. [ Links ]
18. Bischoff -Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson -Hughes B.. Estimation of optimal serum concentration of 25 -hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 2006; 84(1):18 - 28. [ Links ]
19. Grimes DS. Are statins analogues of vitamin D? Lancet 2006; 368(9529):83 -86. [ Links ]
20. Dusso AS, Brown AJ, Slatopolsky E. Vitamin D. Am J Physiol Renal Physiol 2005; 289(1): F8 - 28. [ Links ]
21. Yasmin R, Williams RM, Xu M, Noy N. Nuclear import of the retinoid x receptor, the vitamin D receptor, and their mutual heterodimer. J Biol Chem 2005;280(48):40152 -401 60. [ Links ]
22. Norman AW, Henry HL, Bishpo JE, Song XD, Bula C, Okamura WH. Different shapes of the steroid hormone 1 alpha,25(OH)(2)-vitamin D(3) act as agonists for two different receptors in the vitamin D endocrine system to mediate genomic and rapid responses. Steroids 2001; 66(3 -5):147 -158. [ Links ]
23. Lips P. Vitamin D physiology. Prog Biophys Mol Biol 2006; 92(1): 4 - 8. [ Links ]
24. Nagpal S, Na S, Rathnachalam R. Noncalcemic actions of vitamin D receptor ligands. Endocr Rev 2005; 26(5): 662 - 687. [ Links ]
25. Gurlek A, Pitelkow MR, Kumar R. Modulation of growth factor/cytokine synthesis and signaling by 1α, 25 -dihydroxyvitamin D3: Implications in cell growth and differentiation. Endrocr Rev 2002; 23(6): 763 -7 86. [ Links ]
26. Cohen -Lahav M, Shany S, Tobvin D, Chaimovitz C, Douvdevani A. Vitamin D decreases NFkappaB activity by increasing IkappaBalpha levels. Nephrol Dial Transplant 2006; 21(4):889 - 897. [ Links ]
27. Christakos S, Raval-Pandya M, Wernyj RP, Yang W. Genomic mechanisms involved in the pleiotropic actions of 1,25 -dihydroxyvitamin D3. Biochem J 1996; 316(Pt 2): 361 - 371. [ Links ]
28. Norman AW, Frankel BJ, Heldt AM, Grodsky GM. Vitamin D deficiency inhibits pancreatic secretion of insulin. Science 1980; 209(4458):823 - 825. [ Links ]
29. Harinarayan CV. Vitamin D and diabetes mellitus. Hormones (Athens) 2014; 13(2):163-181. [ Links ]
30. Schneider LE, Schedl HP, McCain T, Haussler MR. Experimental diabetes reduces circulating 1, 25 -dihydroxyvitamin D in the rat. Science 1977; 196(4297):1452 -1454. [ Links ]
31. The NS, Crandell JL, Lawrence JM, et al. Vitamin D in youth with type 1 diabetes: prevalence of insufficiency and association with insulin resistance in the SEARCH Nutrition Ancillary Study. Diabet Med 2013;30(11):1324 -1332. [ Links ]
32. Speer G, Cseh K, Winkler G, et al. Vitamin D and estrogen receptor gene polymorphisms in type 2 diabetes mellitus and in android type obesity. Eur J Endocrinol 2001; 144(4): 385 - 389. [ Links ]
33. Ogunkolade BW, Boucher BJ, Prahl JM, et al. Vitamin D receptor (VDR) mRNA and VDR protein levels in relation to vitamin D status, insulin secretory capacity, and VDR genotype in Bangladeshi Asians. Diabetes 2002; 51(7): 2294 - 2300. [ Links ]
34. Chiu KC, Chu A, Go VL, Saad MF. Hypovitaminosis D is associated with insulin resistance and β cell dysfunction. Am J Clin Nutr 2004; 79(5): 820 - 825. [ Links ]
35. Guo SW, Magnuson VL, Schiller JJ, Wang X, Wu Y, Ghosh S. Meta -analysis of vitamin D receptor polymorphism and Type 1 diabetes: A HuGE review of genetic association studies. Am J Epidemiol 2006; 164(8): 711 - 724. [ Links ]
36. Mattila C, Knekt P, Mannisto S, et al. Serum 25 -hydroxyvitamin D concentration and subsequent risk of type 2 diabetes. Diabetes Care 2007; 30(10):2569 - 2570. [ Links ]
37. Song Y, Wang L, Pittas AG, et al. Blood 25 -hydroxy vitamin D levels and incidente type 2 diabetes. Diabetes Care 2013;36(5):1422 -1428. [ Links ]
38. Hochberg Z, Borochowitz Z, Benderli A, et al. Does 1, 25 -dhydroxyvitamin D participate in the regulation of hormone release from endocrine glands? J Clin Endocrinol Metab 1985; 60(1): 57 - 61. [ Links ]
39. Bland R, Markovic D, Hills CE, et al. Expression of 25 -hydroxyvitamin D3 -1 alpha-hydroxylase in pancreatic islets. J Steroid Biochem Mol Biol 2004; 89 -90(1 -5):121 - 125. [ Links ]
40. Chiu KC, Chu A, Go VL, Saad MF. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am J Clin Nutr 2004; 79(5):820 -825. [ Links ]
41. Al -Daghri NM, Alkharfy KM, Al -Othman A, et al. Vitamin D supplementation as an adjuvant therapy for patients with T2DM: an 18 -month prospective interventional study. Cardiovasc Diabetol 2012; 11(1):85. [ Links ]
42. Davidson MB, Duran P, Lee ML, Friedman TC. High -dose vitamin D supplementation in people with prediabetes and hypovitaminosis D. Diabetes Care 2013;36(2):260-266. [ Links ]
43. Ismail A, Namala R. Impaired glucose tolerance in vitamin D deficiency can be corrected by calcium. J Nutr Biochem 2000; 11(3):170 - 175. [ Links ]
44. Pittas AG, Lau J, Hu FB, Dawson -Hughes B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta -analysis. J Clin Endocrinol Metab 2007; 92(6):2017 - 2029. [ Links ]
45. Bourlon PM, Billaudel B, Faure -Dussert A. Influence of vitamin D3 deficiency and 1,25 dihydroxyvitamin D3 on de novo insulin biosynthesis in the islets of the rat endocrine pancreas. J Endocrinol 1999; 160(1):87 -95. [ Links ]
46. The EURODIAB Substudy 2 Study Group. Vitamin D supplement in early childhood and risk for type I (insulin -dependent) diabetes mellitus. Diabetologia 1999; 42(1): 51 - 4. [ Links ]
47. Giarratana N, Penna G, Amuchastegui S, Mariani R, Daniel KC, Adorini L. A vitamin D analog down -regulates proinflammatory chemokine production by pancreatic islets inhibiting T cell recruitment and type I diabetes development. J Immunol 2004; 173(4): 2280 -228 7. [ Links ]
48. Gnudi L, Thomas SM, Viberti G. Mechanical forces in diabetic kidney disease: A trigger for impaired glucose metabolism. J Am Soc Nephrol 2007; 18(8):2226 -22 32. [ Links ]
49. Ayo SH, Radnik RA, Glass WF 2nd, et al. Increased extracellular matrix synthesis and mRNA in mesangial cells grown high -glucose medium. Am J Physiol 1991; 260(2Pt 2): F185 - 191. [ Links ]
50. Huang C, Kim Y, Caramori ML, et al. Cellular basis of diabetic nephropathy: III. In vitro GLUT1 mRNA expression and risk of diabetic nephropathy in type 1 diabetic patients. Diabetologia 2004; 47(10):1789 -1794. [ Links ]
51. Gnudi L, Viberti G, Raij L, et al. GLUT -1 overexpression: Link between hemodynamic and metabolic factors in glomerular injury? Hypertension 2003; 42(1):19 - 24. [ Links ]
52. Yamamoto T, Nakamura T, Noble NA, Ruoslahti E, Border WA. Expression of transforming growth factor β is elevated in human and experimental diabetic nephropathy. Proc Natl Acad Sci USA 1993; 90(5):1814 - 1818. [ Links ]
53. Leask A, Abraham DJ. TGF -β signalling and the fibrotic response. FASEB J 2004; 18(7): 816 -8 27. [ Links ]
54. Ziyadeh FN. Mediators of diabetic renal disease: The case for TGF -β as the major mediator. J Am Soc Nephrol 2004; 15(Suppl 1):S55 -S57. [ Links ]
55. Brownlee M. The pathobiology of diabetic complications. A unifying mechanism. Diabetes 2005; 54(6):1615 - 1625. [ Links ]
56. Thomas MC, Forbes JM, Cooper ME. Advanced glycation end products and diabetic nephropathy. Am J Ther 2005; 12(6):562 - 572. [ Links ]
57. Leehey DJ, Singh AK, Alavi N, Singh R. Role of angiotensin II in diabetic nephropathy. Kidney Int Suppl 2000; 77:S93 - S98. [ Links ]
58. Mezzano SA, Ruiz -Ortega M, Egido J. Angiotensin II and renal fibrosis. Hypertension 2001; 38(3 Pt 2):635 - 638. [ Links ]
59. Rincon -Choles H, Kasinath BS, Gorin Y, Abboud EH. Angiotensin II and growth factors in the pathogenesis of diabetic nephropathy. Kidney Int Suppl 2002; 82:S8- S11. [ Links ]
60. Liebau MC, Lang D, Bohm J, et al. Funcional expression of the rennin –angiotensin system in human podocytes. Am J Physiol Renal Physiol 2006; 290(3):F710 - F719. [ Links ]
61. Yoo TH, Li JJ, Kim JJ, et al. Activation of the renin -angiotensin system within podocytes in diabetes. Kidney Int 2007; 71(10):1019 - 1027. [ Links ]
62. Haraldsson B, Nystrom J, Deen WM. Properties of the glomerular barrier and mechanisms of proteinuria. Physiol Rev 2008; 88(2):451 - 487. [ Links ]
63. Kelly DJ, Aaltonen P, Cox AJ, et al. Expression of the slit -diaphragm protein, nephrin, in experimental diabetic nephropathy: differing effects of anti -proteinuric therapies. Nephrol Dial Transplant 2002; 17(7):1327 - 1332. [ Links ]
64. Lerco MM, Macedo CS, Silva RJ, Pinheiro Dde O, Spadella CT. The number of podocyte and slit diaphragm is decreased in experimental diabetic nephropathy. Acta Cir Bras 2006; 21(2):87 - 91. [ Links ]
65. White KE, Bilous RW, Marshall SM, et al. Podocyte number in normotensive type 1 diabetic patients with albuminuria. Diabetes 2002; 51(10):3083 -30 89. [ Links ]
66. Fioretto P, Mauer M. Histopathology of diabetic nephropathy. Semin Nephrol 2007; 27(2):195 - 207. [ Links ]
67. Wolf G, Ziyadeh FN. Cellular and molecular mechanisms of proteinuria in diabetic nephropathy. Nephron Physiol 2007; 106(2):26 - 31. [ Links ]
68. Pagtalunan ME, Miller PL, Jumping -Eagle S, et al. Podocyte loss and progressive glomerular injury in type II diabetes. J Clin Invest 1997; 99(2):342 - 348. [ Links ]
69. Schiffer M, Bitzer M, Roberts IS, et al. Apoptosis in podocytes induced by TGF –β and Smad7. J Clin Invest 2001; 108(6):807 - 816. [ Links ]
70. Fowlkes JL, Bunn RC, Cockrell GL, et al. Dysregulation of the Intrarenal Vitamin D Endocytic Pathway in a Nephropathy -Prone Mouse Model of Type 1 Diabetes. Exp Diabetes Res 2011; 7:1155 - 2011. [ Links ]
71. Zhang Z, Yuan W, Sun L, et al. 1,25 –Dihydroxyvitamin D3 targeting of NF - kB suppresses high glucose -induced MCP -1 expression in mesangial cells. Kidney Int 2007: 72(2):193 - 201. [ Links ]
72. Matthias S, Busch R, Merke J, Mall G, Thomasset M, Ritz E. Effects of 1,25(OH)2D3 on compensatory renal growth in the growing rat. Kidney Int 1991; 40(2):212 - 218. [ Links ]
73. Tian J, Liu Y, Williams LA, Zeeuw D. Potential role of active vitamin D in retarding he progression of chronic kidney disease. Nephrol Dial Transplant 2007; 22(2):321-- 328. [ Links ]
74. Zhang Z, Yuan W, Sun L, et al. 1,25–Dihydroxyvitamin D3 targeting of NF – kappaB suppresses high glucose -induced MCP -1 expression in mesangial cells. Kidney Int 2007; 72(2):193 - 201. [ Links ]
75. Alborzi P, Patel NA, Peterson C, et al. Paricalcitol reduces albuminuria and inflammation in chronic kidney disease. A randomized double -blind pilot trial. Hypertension 2008; 52(2):249 - 255. [ Links ]
76. Tan X, Wen X, and Liu Y. Paricalcitol inhibits renal inflammation by promoting vitamin D receptor–mediated sequestration of NF -kappaB signaling. J Am Soc Nephrol 2008; 19(9):1741 -17 52. [ Links ]
77. Kuhlmann A, Haas CS, Gross ML, et al. 1,25-Dihydroxivitamin D3 decreases podocyte loss and podocyte hypertrophy in the subtotally nephrectomized rat. Am J Physiol Renal Physiol 2004; 286(3):F526 -533. [ Links ]
78. Tan X, Li Y, Liu Y. Therapeutic role and potential mechanisms of active Vitamin D in renal interstitial fibrosis. J Steroid Biochem Mol Biol 2007; 103(3 -5):491 - 496. [ Links ]
79. Migliori M, Giovannini L, Panichi V, et al. Treatment with 1,25 -dihydroxyvitamin D3 preserves glomerular slit diaphragm -associated protein expression in experimental glomerulonephritis. Int J Immunopathol Pharmacol 2005; 18(4):779 -790. [ Links ]
80. Xiao HQ, Shi W, Liu SX, et al. Podocyte injury is suppressed by 1, 25 –dihydroxyvitamin D via modulation of transforming growth factor-beta 1/bone morphogenetic protein-7 signalling in puromycin aminonucleoside nephropathy rats. Clin Exp Pharmacol Physiol 2009; 36(7):682 - 689. [ Links ]
81. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1, 25 -Dihydroxyvitamin D(3) is a negative endrocrine regulator of the rennin -angiotensin system. J Clinic Invest 2002; 110(2):229 - 238. [ Links ]
82. Li YC. Vitamin D regulation of the renin -angiotensin system. J Cell Biochem 2003; 88(2):327 - 331. [ Links ]
83. Klaus G. Renoprotection with vitamin D: Specific for diabetic nephropathy? Kidney Int 2008; 73(2):141 -14 3. [ Links ]
84. Agarwal R, Acharya M, Tian J, et al. Antiproteinuric effect of oral paricalcitol in chronic kidney disease. Kidney Int 2005; 68(6):2823 -28 28. [ Links ]
85. Alborzi P, Patel NA, Peterson C, et al. Paricalcitol reduces albuminuria and inflammation in chronic kidney disease: a randomized double -blind pilot trial. Hypertension 2008; 52(2):249 - 255. [ Links ]
86. Szeto CC, Chow KM, Kwan BC, Chung Ky, Leung CB, Li PK. Oral calcitriol for the treatment of persistent proteinuria in immunoglobulin A nephropathy: an uncontrolled trial. Am J Kidney Dis 2008; 51(5):724 - 731. [ Links ]
87. Aperis G, Paliouras C, Zervos A, Arvanitis A, Alivanis P. The role of paricalcitol in proteinuria. J Ren Care 2011; 37(2):80 - 84. [ Links ]
88. de Zeew D, Agarwal R, Amdahl M, et al. Selective vitamin D receptor activation with paricalcitol for reduction of albuminuria in patients with type 2 diabetes (VITAL study). A randomised controlled trial. Lancet 2010; 376(9752):1543 - 1551. [ Links ]
89. Kim MJ, Frankel AH, Donaldson M, et al. Oral cholecalciferol decreases albuminuria and urinary TGF -β1 in patients with type 2 diabetic nephropathy on established rennin-angiotensin -aldosterone system inhibition. Kidney Int 2011; 80(8):851 - 860. [ Links ]
90. Thadani R, Appelbaum E, Pritchett Y, et al. Vitamin D therapy and cardiac structure and function in patients with chronic kidney disease: the PRIMO randomized controlled trial. JAMA 2012; 307(7):674 - 684. [ Links ]
91. Artaza JN, Contreras S, Garcia LA, et al. Vitamin D and cardiovascular disease: potential role in health disparities. J Health Care Poor Underserved 2011; 22(4 Suppl):23 - 38. [ Links ]
92. Manson JE. Vitamin D and the heart: Why we need large-scale clinical trials. Cleve Clin J Med. 2010; 77(12):903 - 910. [ Links ]
93. Neves PL, Malho A, Cabrita A, et al. Statins and vitamin D: a friendly association in pre-dialysis patients. Int Urol Nephrol. 2010; 42(1):173 -17 9 [ Links ]
Dr.a Ana Paula Silva
Department of Nephrology, Hospital de Faro – Centro Hospitalar do Algarve.
Rua Leão Penedo, 8000 -386 Faro, Portugal
E-mail: anapassionara@gmail.com
Conflict of interest statement: None declared.
Received for publication: 15/04/2014
Accepted in revised form: 17/05/2014


{kind=link}
{kind=link}
{kind=link}
{kind=link}