










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.28 no.1 Lisboa Mar. 2014
ORIGINAL ARTICLE
Acute rejection during the first six-months after transplantation: temporal trends regarding risk factors and effects on graft and patient survival
Rejeição Aguda nos primeiros 6 meses pós transplante: tendências temporais dos fatores de risco e efeitos na sobrevida do enxerto e doente
Rui Costa1, Jorge Malheiro2, Clara Santos3, Isabel Fonseca2, La Salete Martins2, Sofia Pedroso2, Manuela Almeida2, Leonidio Dias2, Antonio Castro-Henriques2, Teresa Morgado1, Antonio Cabrita2
1Nephrology Department, Centro Hospitalar de Trás-os-Montes e Alto Douro, Vila Real, Portugal
2Trasplantation Department, Centro Hospitalar do Porto, Oporto, Portugal 3Nephrology Department, CHVNG, Vila Nova de Gaia, Portugal
ABSTRACT
Objective: To determine risk factors for acute rejection in the first 6 months post- transplant and their effect on death-censored graft and patient survival in the 990-1999 and 2000-2009 periods. Patients and Methods: Retrospective analysis of acute rejection episodes was performed separately in two periods: 1990-1999 and 2000-2009. Multivariate logistic regression analysis was performed in order to identify risk factors for acute rejection. Death-censored graft and patient survival comparison between patients with or without acute rejection occurrence was performed by Kaplan-Meier analysis. Multivariate Cox regression analysis identified independent predictors for death-censored graft and patient survival, assuming the following model: acute rejection, patients age (< 40 vs. ≥ 40 years) and gender, time on haemodialysis / peritoneal dialysis (< 36 vs. ≥ 36 months), live vs. deceased donor (only after the year 2000), HLA mismatches (0-3 vs. 4-6), PRA (≤ 15 vs. > 15%), number of previous kidney transplants (< 2 vs. ≥ 2), status of hepatitis B/C, donor´s age (< 38 vs. ≥ 38 years) and gender, delayed graft function (DGF), ATG use in induction immunosuppression (IS), MMF or Tacrolimus use in induction / maintenance IS (after 2000). Results: A total of 1299 kidney transplants were analyzed. Acute rejection was more frequently diagnosed in the 1990s (26.2% vs. 11.1%, p < 0.001). Over this period, ATG non-use (OR 1.88, p = 0.025) and patients age < 40 years (OR 2.39, p = 0.001) were risk factors for AR while, after 2000, DGF (OR 1.895, p = 0.046) and PRA > 15% (OR 3.519, p = 0.001) were identified. Five years death-censored graft survival was lower in AR cases in the 1990s (81% vs. 94%, p < 0.001) and after 2000 (81% vs. 91%, log rank p = 0.004). Independent predictors for worse death-censored graft survival in 1990-1999 patients were AR (HR 2,436, p < 0.001), patient´s age < 40 years (HR 1.984, p = 0.002) and donor´s age ≥ 38 years (HR 1.961, p = 0.002), while after 2000, DGF (HR 3.247, p < 0.001) and donor´s age ≥ 38 years (HR 2.32, p = 0.017) were identified. No difference was found at five-year patient survival in both groups. Only hepatitis B/C (HR 1.714, p = 0.023) was identified as an independent predictor for patient death in the 1990-1999 period, while after 2000, retransplantation (HR 2,718, p = 0.049) and AR (HR 2,619, p = 0.023) were determinant. Conclusion: After the year 2000, AR was no longer an independent predictor for poor graft survival. Inversely, AR began to play a deleterious effect on patient survival. Advances on immunosuppressive drugs allowed the increase of kidney transplant on hypersensitized patients, with improvement of graft survival in those patients but also with a possible deleterious effect on patient survival.
Key-words: acute rejection; kidney transplant; predictors; survival.
RESUMO
Objetivo: Avaliar na década de 90 e 2000 os fatores preditores de rejeição aguda (RA) aos 6 meses pós transplante renal (TR) e o seu efeito na sobrevida censurada do enxerto e do doente. Material e Métodos: Análise retrospetiva dos casos de RA efetuada separadamente em dois períodos: 1990-1999 e 2000-2009. Na avaliação dos fatores de risco para RA foi utilizado um modelo de regressão logística multivariada. Procedemos à construção de curvas comparativas de sobrevivência do enxerto entre paciente com e sem RA pelo método de Kaplan-Meier em cada período. A regressão de Cox multivariada permitiu identificar os preditores de sobrevivência censurada do enxerto e doente, usando como modelo: rejeição aguda, idade (< 40 vs ≥ 40 anos) e sexo do recetor, tempo em HD/DP (< 36 vs. ≥ 36meses), dador vivo vs. cadavérico (apenas na década de 2000), incompatibilidades HLA (0-3 vs. 4-6), PRA (≤ 15 vs. > 15%), número de TR prévios (< 2 vs. ≥ 2), status de hepatite B/C, idade (< 38 vs. ≥ 38 anos) e sexo do dador, episódio de necrose tubular aguda (NTA), uso de ATG na imunossupressão (IS) de indução, uso de MMF ou Tacrolimus (apenas na década de 2000) na IS de indução/manutenção. Resultados: Num total de 1299 transplantes renais, 644 (49.5%) foram realizados na década de 90 e 655 (50.5%) na década de 2000. A RA foi mais frequente na década de 90 (26.2% vs. 11.1%, p < 0.001). Nesta década, os fatores de risco para RA foram o não-uso de ATG (OR 1.88, p = 0.025) e a idade do recetor < 40 anos (OR 2.39, p = 0.001). Na década de 2000, NTA (OR 1.895, p = 0.046) e PRA > 15% (OR 3.519, p = 0.001) foram os fatores de risco identificados. A sobrevivência censurada do enxerto aos 5 anos foi inferior nos casos de RA na década de 90 (81% vs. 94%, p < 0.001) e 2000 (81% vs. 91%, log rank p = 0.004). Na análise de regressão Cox, os preditores de menor sobrevivência do enxerto na década de 90 foram a RA (HR 2,436, p < 0.001), idade do recetor < 40 anos (HR 1.984, p = 0.002) e idade do dador ≥ 38 anos (HR 1.961, p = 0.002). Na década de 2000 foram identificadas a NTA (HR 3.247, p < 0.001) e idade de dador ≥ 38 anos (HR 2.32, p = 0.017). Não encontramos diferenças na sobrevida do doente aos 5 anos em ambos períodos. Apenas o status de Hepatite B/C (HR 1.714, p = 0.023) foi preditor independente de morte do doente na década de 90, enquanto que na década de 2000, os preditores significativos foram TR prévio (HR 2,718, p = 0.049) e RA (HR 2,619, p = 0.023). Conclusão: A partir de 2000, a RA aos 6 meses deixou de ser um preditor independente de sobrevivência do enxerto. Inversamente, passou a ter um efeito negativo independente na sobrevivência do doente. Os avanços na IS permitiu o TR em recetores cada vez mais sensibilizados, com melhoria na sobrevida do enxerto nestes casos mas com possível efeito desfavorável na sobrevida do doente.
Palavras chave: preditores; rejeição aguda; sobrevida; transplante renal.
INTRODUCTION
Acute rejection (AR) episodes in renal transplantation are known to be one important negative prognostic factor for short- and long-term graft survival. Efforts in preventing these early events were considered crucial in order to increase graft survival. The improvement of the short-term transplantation results during the last two decades is largely due to a progressive decrease in the incidence and better management of AR episodes, mostly explained by introduction of better immunosuppressive therapies. Despite these beneficial effects on early graft survival, significant improvement on overall graft survival is still not observed1. Possibly, the previous negative impact of AR episodes on long-term graft survival is currently being replaced by the negative effect of chronic rejection mechanisms. Moreover, it is possible that rejection events may present different effects on graft survival according to their severity or time of presentation2,3.
Accordingly, better knowledge of risk factors for AR is crucial for the implementation of prophylactic measures and acute event management.
With the present study, we analyzed separately the periods 1990-1999 and 2000-2009 in regard to incidence of early AR episodes, independent risk factors for their occurrence, and subsequently proceeded to investigate whether AR has independent deleterious effect on patient and graft survival, in our Centre, in both periods.
PATIENTS AND METHODS
We performed a retrospective analysis of all kidney transplants performed in our Centre in two separate periods: 1990-1999 and 2000-2009. For each period, clinical data regarding patient gender and age at the time of transplantation, cumulative time on haemodialysis (HD) or peritoneal dialysis (PD), chronic hepatitis B or C infection, number of previous renal transplants, HLA A, B and DR mismatches, panel reactive antibody (PRA), donor age and gender, use of anti-thymocite globuline (ATG) in induction immunosuppression (IS) and delayed graft function (DGF) was obtained. Deceased or live donor and use of tacrolimus (TAC) and mycophenolate mofetil (MMF) in induction or maintenance immunosuppression were only considered after the year 2000. Acute rejection episodes based on biopsy-proven diagnosis were only considered when occurring within the first six months post-transplantation. To examine the impact of AR, comparison of patient and deathcensored graft survival during a 10-year follow-up between subjects, with or without acute rejection, in each period was performed using Kaplan Meier analysis with strata comparisons measured by logrank test.
Multivariate analysis was performed based on the following model: acute rejection, patient gender and age at transplantation (< 40 vs. ≥ 40 years), donor gender and age (< 38 vs. ≥ <38 years), time on HD/PD (< 36 vs. ≥ 36 months), HLA mismatch (0-3 vs. 4-6), PRA (< 15 vs. ≥ <15 %), previous renal transplant (< 2 vs. ≥ 2), chronic hepatitis B or C infection, deceased / live donor, ATG use in induction IS, TAC and MMF use in induction and maintenance IS and DGF. In each period, two tails chi-square test was applied to test the differences between the groups. Determination of independent risk factors for acute rejection was performed by multivariate logistic regression and patient and death-censored graft survival in relation to rejection episodes were analyzed using the Cox proportional hazards regression model. The significance level was 0.05 for all statistical tests.
RESULTS
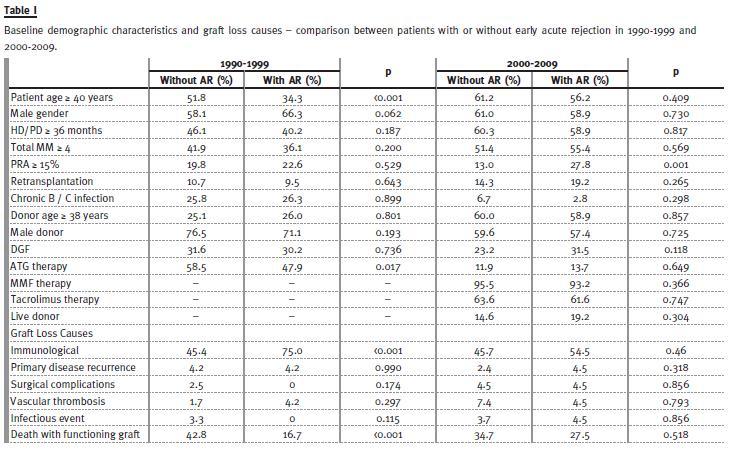
From a total of 1299 patients analyzed, equal distribution between 1990-1999 (n = 645) and 2000-2009 (n = 654) was found. Early AR was experienced by 242 patients (18.4%) and significant temporal decrease on rejection between both periods was found (26.2 vs. 11.1% p < 0.011). The baseline characteristics of patients with or without rejection event in each period are summarized in Table I. In the first period analyzed (1990-1999), the rejection group of patients were younger (patient age ≥ 40 years: 34.3 vs.51.8%, p < 0.001) and lesser ATG use in induction IS was found (47.9 vs. 58.5 %, p = 0.017). After 2000, AR patients presented higher PRA (PRA ≥ 15%: 27.8% vs. 13.0%, p = 0.001). Eighteen patients presented PRA ≥ 50%, mostly after 2000 (n = 12). In both periods, no differences regarding the other variables were found. The multivariate logistic regression model was applied to both periods in order to determine factors that significantly increased the risk of AR. In the 1990-1999 group, the age of patients was under 40 years (OR 2.39, p = 0.001) and IS without ATG (OR 1.88, p = 0.025) were found to have an independent role on AR occurrence. When transplants performed in 2000-2009 were evaluated by logistic regression analysis, sensitized patients (PRA ≥ <15%: OR 3.52, p = 0.001) and occurrence of DGF (OR 1.89, p = 0.046) were identified.
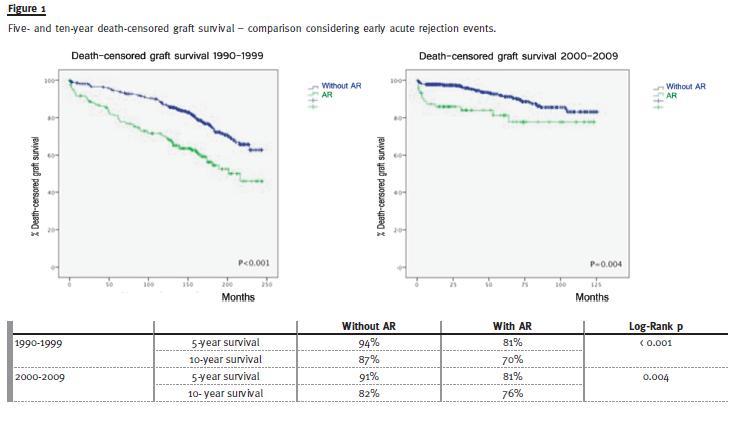
Univariate analysis for causes of graft loss in both periods is displayed in Table II. In the 1990-1999 group, immunological mechanisms caused most graft losses, especially in AR patients (75% vs. 45.4%, p < 0.001), while no differences were found in 2000-2009. In order to investigate the impact of AR on long-term graft survival, death-censored graft survival at 5- and 10-year follow-up was determined (Figure 1). Grafts with AR episodes were associated to a worse graft survival in both periods. In the1990-1999 period, 5-year survival was 81% (vs. 94%) and 10-year survival was 70% (vs. 87%, long rank p = 0.001).
When the Cox hazard model estimates was applied on this period, independent predictors for poor death-censored graft survival identified were AR (HR 2.44, p < 0.001), patient´s age under 40 years (HR 1.98, p = 0.002) and donor age over 38 years (HR 1.96, p = 0.002).
As displayed in Fig 1, the AR group was also associated to worse 5-year (81% vs. 91%) and 10-year death-censored graft survival (76% vs. 82%, long rank p = 0.004) concerning the period 2000-2009.
In these patients, independent predictors identified for worse graft survival were DGF (HR 3.25, p < 0.001) and donor age over 38 years (HR 2.32, p = 0.017), while AR occurrence did not shown independent deleterious effect on graft survival (HR 1.59, p = 0.221). However, in further sub analysis performed considering graft loss events during the first year in this period (n = 23), AR appears as independent predictor for graft loss (HR 2.3, p < 0.04) In these patients, occurrence of first year graft loss was also associated to PRA ≥ <15% (17% vs. 3%, p = 0.01).
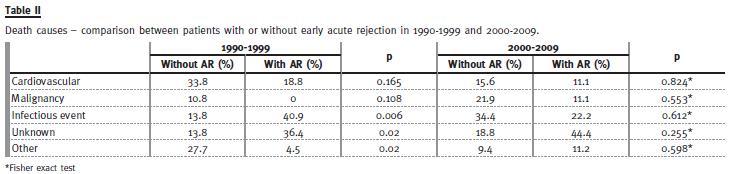
Death causes due to infectious, cardiovascular, malignancy or others events (including trauma, gastrointestinal, surgical pathologies) are described in Table II. In 1990-1999 patients who experienced AR, association between infectious events and patient death was found (40.9% vs. 13.8%, p < 0.01), while no difference was detected in 2000-2009 patients.
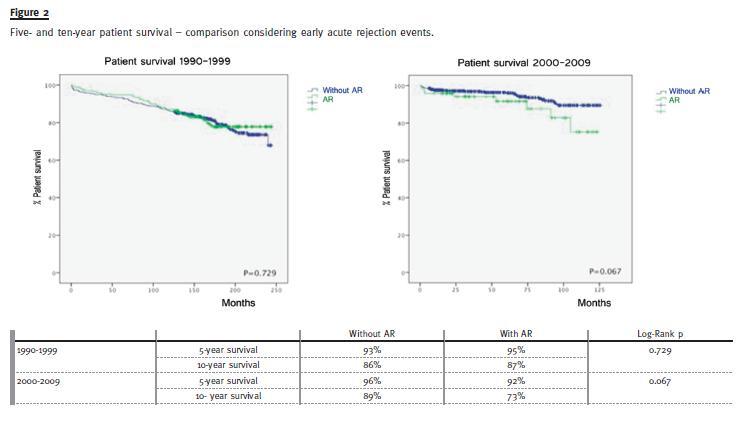
Ten-year patient survival was also analyzed (Fig. 2) and, in both periods, no statistical difference was found between patients with or without AR episodes, although 2000-2009 patients that experienced AR tended to present lower survival (73% vs. 89%, p = 0.067). Cox hazards model was applied to each period in order to determine independent predictors for patient survival. Beneath the obvious effect of patient older age, hepatitis B or C infection predicted lower patient survival in 1990-1999 (HR 1.71, p = 0.02), while retransplantation was associated to increased risk for lower survival in 2000-2009 patients (HR 2.72, p = 0.049). Only in this latter period, AR was identified as a deleterious independent predictor for patient survival (HR 2.62, p = 0.023).
DISCUSSION
This analysis was performed to evaluate the changing profile of early acute rejection (during the first 6 months) on kidney transplant recipients and its repercussions on late transplant and patient survival over the last 20 years in our Centre. A major finding was the marked reduction in the incidence of AR observed in kidney transplants performed in 2000-2009 compared with those performed in 1990-1999, coinciding with the introduction of TAC and MMF therapy. As described in other reports4,5, acute rejection rates have progressively decrease, probably due to the evolution of immunosuppressive regimens, especially after Tacrolimus and MMF introduction. Tacrolimus is believed to cause lower incidence of acute rejection when compared to cyclosporine, while other recent reports defend that acute rejection rates between tacrolimus and cyclosporine are generally similar, given the growing adoption of induction therapy with IL-2 receptor inhibitor6. Nevertheless, combination therapy Tacrolimus/MMF has shown to improve lower incidence of acute rejections when compared to cyclosporine/ MMF7. Accordingly, most of our patients started Tacrolimus / MMF therapy in our Centre in 2000 and this fact may have contributed for the AR reduction observed since then.
Induction therapy with lymphocyte-depleting agent is known to reduce acute rejection, especially in high-immunological-risk patients8. Accordingly, our results concerning the first period analyzed, the non-use of ATG in induction therapy was associated to increased risk for AR. As has been reported in other series9, we also observed an increased risk of acute rejection in younger recipients, but only in the first period studied (1990-1999). According to UNOS Scientific Renal Transplant Registry (1999)10 regarding transplants performed in a similar period (between 1994 and 1998), an increased risk for immunological graft loss in younger patients was found. Higher donor/receptor age difference, lack of therapy adherence and higher immunological reactivity may explain these results. The increasingly higher proportion of older patients submitted to kidney transplant and the improvement of immunosuppressive protocols, allowing therapeutic individualization and better adherence, may explain the absence of higher risk for AR in younger patients in our second period (2000-2009).
Besides identical ABO and time on dialysis, the Portuguese kidney allocation system from deceased donors implemented extra points attribution to hyper immunized patients (PRA > 50%) since 2007, in order to reduce their long cumulative time on dialysis.
However, the presence of antibodies to a broad panel of potential donors is known to increase risk of acute rejection, which can be minored with actual desensitization protocols11. Indeed, we found higher risk for AR in patients presenting PRA ≥ 15% only in 2000-2009, suggesting a temporal trend to higher number of patients with higher immunological risk being allocated for transplantation. The limited organs available for transplantation, the increasing number of retransplantations and patients on dialysis waiting for a renal allograft has led to higher proportion of hypersensitized patients submitted to transplantation.
Most delayed graft function cases are a consequence of acute tubular necrosis (ATN). This ischemic injury depends on donor age and condition and begins right before the removal of the organs, during the time of cold ischemia in preservation fluid, prolonged warm ischemia time during surgery and any hypotensive episodes following implantation.
Adding to this, the kidney is almost always affected by ischemia- reperfusion injury, which results from the high concentration of oxygen free radicals formation after oxygen becomes available to cells previously under anaerobic metabolism. The ischemic injury leads to endothelial injury, resulting on upregulation and exposure of donor histo-compatibility antigens, adhesion and costimulatory molecules12, increasing the risk for acute rejection. Previous studies have reported increased risk for AR in DGF patients: Javaram et al.13 have shown that DGF patients with more than one-time dialysis requirement displayed higher incidence of acute rejection during the first year (OR 1.66, p = 0.015). The association between DGF and acute rejection was also shown in our results, presenting similar results in 2000-2009, where occurrence of DGF increased AR risk by 89%.
Although univariate comparison regarding deathcensored graft survival showed worse prognosis in grafts that experienced rejection in both periods, only in the first (1990-1999) was found an independent deleterious role of AR on graft survival. In the same period, graft loss due to immunological mechanisms was associated to previous AR events. There is growing evidence that multiple factors related to the rejection episode itself play a role in determining long-term consequences. Number, type, severity, reversibility and timing of rejection could be identified as determinants of renal graft survival.
First, the functional response of the acute rejection episode to therapy is important to determine which will have impact on graft survival and which will not. Vereerstraeten et al14 analysed rejection episodes that occurred during the first year post-transplant and compared long-term graft survival without rejection episodes, rejection without loss of graft function and rejection with partial or total function loss. Their results showed that rejection episodes without loss of graft function do not exert a detrimental influence on long-term survival. Opelz et al3 also demonstrated that AR followed by partial loss of graft function exerts a more detrimental effect on long-term outcome than rejection with total recovery. Additionally, within the same study, the authors show that late AR (after one year posttransplant) are usually more difficult to reverse by anti-rejection therapy than early events and, consequently, are associated to worse death-censored graft survival.
Despite AR incidence reduction, overall long-term graft survival remained constant in our study. This discordance between trend in acute rejection rates and in long-term graft survival has been observed in other studies1, implying that achievement of lower rejection rates does not necessarily improve graft survival. Another intriguing fact is that AR no longer showed independent deleterious impact on graft survival in the 2000-2009 study-periods. Acute rejection was identified as risk factor for censured graft loss at the first year after transplantation, especially in patients with PRA ≥ 15%, but this effect was diluted when considering all follow-up time because of the small number of episodes (n = 23). Thus, despite the severity of these events, they occur less frequently. Early episodes are nowadays better prevented and managed. In the majority of cases no immediate graft function loss occurs, so the AR event itself may not necessarily predict lower graft survival. However, these patients may present higher risk for late development of chronic antibody-mediated rejection, leading to worse longterm graft survival. Early AR patients present also higher risk for repeat rejection episodes during graft lifetime, which can cause subsequent cumulative allograft damage. Additionally, effects related to over- immunosuppression, like polyomavirus nephropaty or other infectious events, graft toxicity and metabolic disorders, can also contribute to lower long-term graft survival. Other potential reasons might include the increasing transplantation procedures in higher risk recipients and older donors in more recent years.
Patient survival after transplantation depends on the source of the allograft (live vs. deceased donor), patients age, gender, ethnic origin and presence and degree of co-morbid conditions. Most deaths are attributed to cardiovascular disease, especially in older and diabetic patients, while other life threatening disorders, like infection and malignancy, are responsible for death cases in younger patients15. Other probable contributor factor for patient survival is the overall level of immunosuppression used for induction and maintenance therapy and treatment of acute rejection episodes, which can lead to increased risk of post-transplant infections. Accordingly, graft dysfunction caused by acute rejection and post-transplant infectious episodes is closely interrelated through the use of immunosuppression therapy. Our findings demonstrate that infectious events were responsible for the majority of deaths in patients who experienced rejection episodes only in the 1990-1999 period.
The higher incidence of acute rejection during this period, especially in younger patients, may explain these results. In what concerns the death causes in the 2000-2009 period, no major conclusions can be drawn because the specific death cause was not determined in almost half the patients that experienced rejection. Nevertheless, the decrease of infection-related mortality may be explained by improved preventive measures for severe lifethreatening events, based on prophylactic and preemptive protocols for bacterial and viral infections, regular monitoring for asymptomatic infections and immunosuppressive therapy adjustments during and after infectious episodes.
In our 2000-2009 analysis, acute rejection group tended to present lower patient survival during the 10-year follow-up. Our results suggest that acute rejection may contribute for worse patient prognosis only in this period, as well as retransplantation.
However, only half the patients (n = 39) maintained follow-up after 5 years, leading to statistical bias responsible for higher decreases on cumulative patient survival analysis after each event. Trébern-Launay et al.16 showed that a second renal transplant presented higher risk for acute rejection and was also associated to lower patient- and graft-survival compared to first transplants, but this risk excess was delayed after several years post-transplantation.
However, after considering only patient survival, the authors found no statistical difference despite tendency for lower survival on second transplant patients was observed. We hypothesize that acute rejection episodes and retransplantation are surrogates markers for worse baseline prognosis in allocated patients for transplantation in recent years.
Cumulative time of end-stage renal disease (with increased prevalence of cardiovascular disease), higher immunological risk and overall immunosuppression therapy performed (increased risk for infectious and malignancy events) may be important contributors for poor patient prognosis associated to retransplantation and previous acute rejection.
So, acute rejection episodes may be considered as an alarm sign, targeting patients that present baseline increased risk for a poor outcome.
General conclusions cannot be extrapolated based on this study since it has the limitation of relying on retrospective analysis in a single centre. Careful analysis should be performed regarding the 2000-2009 period, since the Portuguese kidney allocation system changed during this period (2007), favouring kidney transplant on high sensitized and long-term dialysis patients. By this manner, this group is constituted by heterogeneous patients, with different baseline prognosis and acute rejection predisposition.
Additionally, the lack of information regarding the type of rejection (steroid sensitive, steroid resistant or antibody-mediated) and the significant number of cases with unknown death cause are another drawback.
In summary, our results showed a decrease in the incidence of acute rejection in the last 20 years, but risk factors for this event have evolved. Patients with PRA ≥ 15% and delayed graft function were identified as actual independent predictors for early rejection episodes. After 2000, acute rejection was not identified as an independent predictor for lower graft survival but was associated to worse patient prognosis. Baseline characteristics in relation to the increasing number of high sensitized patients, second kidney transplant and cumulative time of end-stage renal disease may contribute to these results.
References
1. Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 2004;4(3):378-383 [ Links ]
2. Madden RL, Mulhern JG, Benedetto BJ, et al. Completely reversed acute rejection is not a significant risk factor for the development of chronic rejection in renal allograft recipients. Transpl Int 2000;13(5):344-50. [ Links ]
3. Opelz G, Döhler B, Collaborative Transplant Study Report. Influence of time of rejection on long-term graft survival in renal transplantation. Transplantation 2008;85(5):661-666 [ Links ]
4. Rockville MD. Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of transplant Recipients: Transplant Data 1998-2007. U.S. Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, 2008 http://www.srtr.org/annual_Reports/default.aspx (accessed 3 June 2013) [ Links ]
5. Macário F, Sociedade Portuguesa de Transplantação. Actividade da Transplantação em Portugal. http://www.spt.pt/index.php?lop=conteudo&op=149e9677a5989fd342ae44213df68868 (accessed 3 June 2013) [ Links ]
6. Nashan B. Is acute rejection the key predictor for long-term outcomes after renal transplantation when comparing calcineurin inhibitors? Transplantation Rev (Orlando) 2009;23(1):47-52 [ Links ]
7. Leichtman AB. Balancing efficacy and toxicity in kidney-transplant immunosuppression. N Engl J Med 2007;357(25):2625-2627 [ Links ]
8. Pallardó Mateu LM, Sancho Calabuig A, Capdevila Plaza L, Franco Esteve A. Acute rejection and late renal transplant failure: risk factors and prognosis. Nephrol Dial Transplant 2004;19 Suppl 3:iii38-iii42 [ Links ]
9. Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant 2009; 9 Suppl 3:S1–S157. [ Links ]
10. Cecka JM. The UNOS Scientific Renal Transplant Registry. Clin Transpl 1999;1-21 [ Links ]
11. Keven K, Sengul S, Celebi ZK, et al. Kidney transplantation in immunologically highrisk patients. Transplant Proc 2013;45(3):919-922 [ Links ]
12. Donovich GM. Handbook of Kidney Transplantation, 5th ed, Philadelphia: Lippincott Williams & Wilkins Handbook Series 2010. [ Links ]
13. Javaram D, Kommareddi M, Sung RS, Luan FL. Delayed graft function requiring more than one time dialysis treatment is associated with inferior clinical outcomes. Clin Transplant 2012;26(5):E536-543 [ Links ]
14. Vereerstraeten P, Abramowicz D, De Pauw L, Kinnaert P. Absence of deleterious effect on long-term kidney graft survival of rejection episodes with complete functional recovery. Transplantation 1997;63(12):1739-1743 [ Links ]
15. Briggs JD. Causes of death after renal transplantation. Nephrol Dial Transplant 2001;16(8):1545-1549 [ Links ]
16. Trébern-Launay K, Foucher Y, Giral M, et al. Poor long-term outcome in second kidney transplantation: a delayed event. PLoS One 2012;7(10):e47915 [ Links ]
Dr. Rui Miguel Costa
Department of Nephrology
Centro Hospitalar de Trás-os-Montes e Alto Douro, Avenida da
Noruega, Lordelo 5000- 508. Vila Real, Portugal
E-mail: ruimiguelccosta@gmail.com
Conflict of interest statement: None declared.
Received for publication: 08/09/2013
Accepted in revised form: 04/12/2013


{kind=link}
{kind=link}
{kind=link}
{kind=link}