










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versión impresa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.4 Lisboa dic. 2013
CASE REPORT
New onset of mixed cryoglobulinemia vasculitis after persistent hepatitis C virus eradication
A propósito de um caso clínico de vasculite crioglobulinémica mista após erradicação persistente do vírus da hepatite C
Rui Andre Silva, Beatriz Malvar, Ricardo Santos, Pedro Pessegueiro, Joao Aniceto, Vitor Ramalho, Manuel Amoedo, Carlos Pires
Nephrology Department, Hospital do Espírito Santo. Évora, Portugal
ABSTRACT
Introduction: Since its identification, hepatitis C virus infection has been implicated in the pathogenesis of several B cell disorders, specifically mixed cryoglobulinemia. Case Report: The authors describe the case of a 41-year-old male, who developed a mixed cryoglobulinemia vasculitis with renal involvement, several years after successful eradication of HCV with interferon therapy. discussion: Similar cases described in the literature are reviewed in this report. Possible explanations for the physiopathology of the disease and its implications in therapy are commented.
Key-Words: B cell; hepatitis C virus; membranoproliferative glomerulonephritis; mixed cryoglobulinemia.
RESUMO
Introdução: Desde que foi identificado, o vírus da hepatite C tem sido implicado na fisiopatologia de diversas doenças linfoproliferativas do tipo B, nomeadamente na criogloblulinemia mista. Caso clínico: Descrevemos o cas crioglobulinemia mista com envolvimento renal, apesar de prévia erradicação do VHC. Discussão: Revemos casos similares descritos na literatura, assim como a fisiopatologia e tratamento desta entidade clínica.
Palavras-chave: célula B; crioglobulinémia mista; glomerulonefrite membranoproliferativa; vírus da hepatite C.
INTRODUCTION
Hepatitis C virus (HCV) infection is a major public health problem, being one of the leading causes of end-stage liver disease and a major liver transplant indication. Additionally, it is also associated with a variety of extrahepatic manifestations, some of them life-threatening1. Hepatitis C virus is the most common cause (50-90%) of mixed cryoglobulinemia (MC), a systemic vasculitis that may involve skin, musculoskeletal system, kidneys and nervous system2. The most frequent type of cryoglobulinemia in patients with HCV is type II MC, which is characterized by polyclonal IgG immunoglobulin linked with a monoclonal antigloblulin, usually IgM class, that acts as an anti-IgG rheumatoid factor. Renal manifestations range from isolated mild proteinuria with microscopic haematuria to an acute full blown nephritic syndrome with renal insufficiency. Type 1 membranoproliferative glomerulonephritis is the most common histological pattern of kidney biopsy in these patients3. The B cell lymphoproliferative diseases are another frequent association with HCV infection.
Prior to the association of HCV, treatment of MC syndrome generally consisted of glucocorticoids, cytotoxic agents and plasmapheresis, typically described as transiently effective and with significant adverse effects3-4. Later, targeted therapy with antiviral treatment, such as interferon alpha (INF-a) or with PEGylated interferon alpha (PEG-INF-a) plus ribavirin provided a new approach to HCV related MC, proved to be much more successful at achieving remission5-6. Recently, with better understanding of HCV lymphotropism and related expansion of rheumatoid factor positive B cell population, therapy with rituximab (RTX), an anti-CD20 monoclonal antibody that depletes B cell population, has been successfully used in the treatment of severe, resistant or relapsing MC7-8.
There has been a strong correlation between antiviral and vasculitic response, shown in virtually all studies. Sustained virologic responses have been connected with effective and enduring remissions.
Quite the opposite, recurrence of symptoms attributable to MC is often paralleled by recurrence of detectable viral replication in those previously treated for HCV5-8. However, there are some cases of persistence of MC syndrome despite demonstration of effective HCV eradication. These cases suggest that HCV infection plays a role in the early activation and proliferation of autoreactive B cell population, but other biological mechanisms may be involved in the maintenance of MC disease in these patients9.
We present a case of new onset MC vasculitis with renal involvement after persistent HCV eradication and discuss the possible underlying mechanisms with a brief literature review.
CASE REPORT
A 38-year-old Caucasian male, heroin addicted, was first diagnosed with HCV infection (genotype 1a) after evaluation due to elevated aminotransferase levels. At this time, he had no extrahepatic manifestations and his hepatic biopsy was suggestive of chronic hepatitis infection. Hepatitis C virus replication activity was detected by HCV RNA quantification (real-time PCR assay, Roche) with viral load of 2,920,000 IU/mL. He received a successful 12-month course of PEG-INF-α and sustained viral response was obtained (no detectable virus for a sensitivity of < 15 IU/mL). Additionally, he abandoned drug consumption and was enrolled in a detoxification programme with methadone.
Three years later, the patient was referred to a nephrology consult due to a hypertensive crisis. He had returned to drug addiction three months earlier, and complained of macroscopic haematuria, lower limb oedema and fatigue. At clinical examination we observed a purpuric rash in his legs and feet dorsum.
Laboratory results showed renal insufficiency (SCr 2,6 mg/dL) with nephrotic proteinuria (15 g/day) and red cell casts. He also presented with anaemia (Hb 8.4 g/dL), hypocomplementemia [C3 33 mg/dL (normal range 90-180); C4 8 mg/dL (normal range 10-40)], normal aminotransferase levels and undetectable HCV RNA or cryoglobulins.
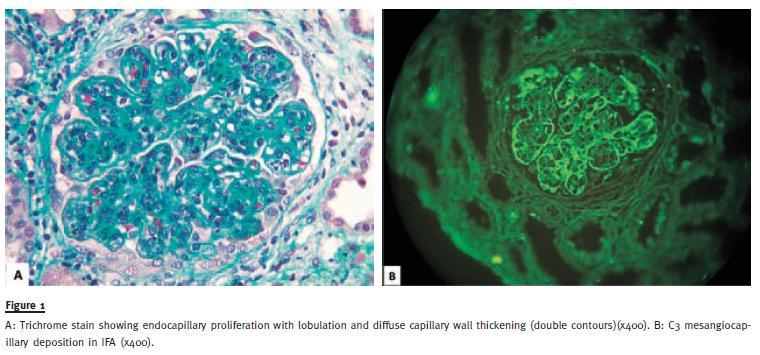
Kidney biopsy was performed and histology was compatible with type I MPGN (Fig. 1): diffuse endocapillary proliferation which results in a lobular appearance and diffuse capillary wall thickening with subendothelial deposits at light microscopy. Mesangiocapillary deposition of IgM, IgG and C3 were present at immunofluorescence. Only at the third attempt, type II IgM/k cryoglobulins were detected, confirming MC disease with renal involvement despite sustained HCV eradication.
The patient returned to drug detoxification programme and was treated with methylprednisolone pulse therapy (1 g/day for 3 consecutive days), followed by prednisone 1mg/Kg/day. After one week of treatment, a response was obtained with disappearance of cutaneous rash, severe reduction of urinary protein excretion (2 g/day) and partial recovery of renal function (SCr 1,8 mg/dL). One month later the patient had markedly improved his renal function (SCr 1.0 mg/dL). At three months, while tapering glucocorticoids, the patient maintained normal renal function, without any MC vasculitis manifestations or cryoglobulins. HCV RNA replication was still undetectable.
During that time, alternative conditions that could predispose to cryoglobulinemia after HCV eradication were excluded, namely, autoimmune diseases, other infectious diseases or a malignant lymphoproliferative disease.
Mucosa associated lymphoid tissue (MALT) lymphoma was excluded by normal upper and lower gastrointestinal endoscopies and accessory salivary gland biopsy. Unfortunately, four months after initial diagnosis, the patient resumed his drug addiction and was lost for follow-up by abandonment. Further investigation of underlying malignant lymphoproliferative disorder was, therefore, impossible.
DISCUSSION
We describe a very unusual case of de novo mixed cryoglobulinemia syndrome with renal involvement after long-term successful HCV eradication, without any evidence of underlying lymphoproliferative malignant disease.
Despite the knowledge about the risk of vasculitic symptoms exacerbation with INF treatment10, the first report of onset cryoglobulinemic vasculitis after initiation of INF therapy was done by Beuthien et al.11. In this case, the MC was diagnosed ten months after the beginning of PEG-INF treatment for HCV; at that time, HCV RNA was undetectable, however, the patient was still undergoing INF therapy, which could be implicated in a vasculitic response, which did not occur in our case.
Levine et al.12 described four patients developing symptomatic cryoglobulinemia regardless of sustained HCV eradication after antiviral therapy. Those patients experienced a relapse of MC during the first year after therapy withdrawal, with rising cryoglobulin levels despite HCV RNA negativity. In all but one, exhaustive search for lymphoproliferative malignant disorders and also HCV RNA PCR analysis on cyoprecipitates was performed, but the results were negative. This report was complemented by an interesting study from Landau et al.13 about eight patients who experienced relapse of HCV associated MC, despite sustained viral response to antiviral treatment.
In all patients, HCV RNA replication was undetectable both in sera and cryoprecipitates. In this study, relapse occurred early after the end of treatment and was usually mild and brief, with only one case of nephropathy. In two of the three patients who had persistent symptoms of vasculitis and high levels of cryoglobulins, B cell lymphoma was diagnosed and only after chemotherapy vasculitis remission was achieved. Both studies highlighted the possibility of cryoglobulinemia syndrome relapsing after successful HCV eradication and contributed to the belief that, as in other autoimmune diseases14, in HCV associated MC, the pathogenic events involving the immune system downstream by the triggering infection, may become independent from the initial stimulus.
Another proposed explanation to these phenomena could be the possibility that despite sustained viral response there may exist viral replication, supported by the demonstration of persistent small quantities of HCV RNA in peripheral blood mononuclear cells (PBMCs), as well as in the liver of patients with a sustained viral response15,16. In fact, Landau et al. used the most sensitive method available to date for the detection of HCV RNA in their report, and still it was negative, which significantly reduced the likelihood that active viral replication had been the cause of MC vasculitis relapse.
Finally, Quartuccio et al.17 reported a case quite similar to ours, of new onset of MC four years after persistent HCV eradication. Yet, the unique feature of our case was the severe renal involvement manifested by an acute nephritic/nephrotic syndrome with membranoproliferative histology.
All these cases suggest a relationship between HCV and B cells. In fact, soon after its discovery, it was shown that HCV was a lymphotropic virus18 and consequently with a connection between HCV infection and lymphoproliferative disorders, mainly MC and B cell non-Hodgkins lymphomas (NHL). This was supported by strong evidence on epidemiological studies that have shown higher risk of NHL development in HCV patients19,20 and demonstrated that effective antiviral therapy can induce haematological remissions in patients with HCV-related NHL21.
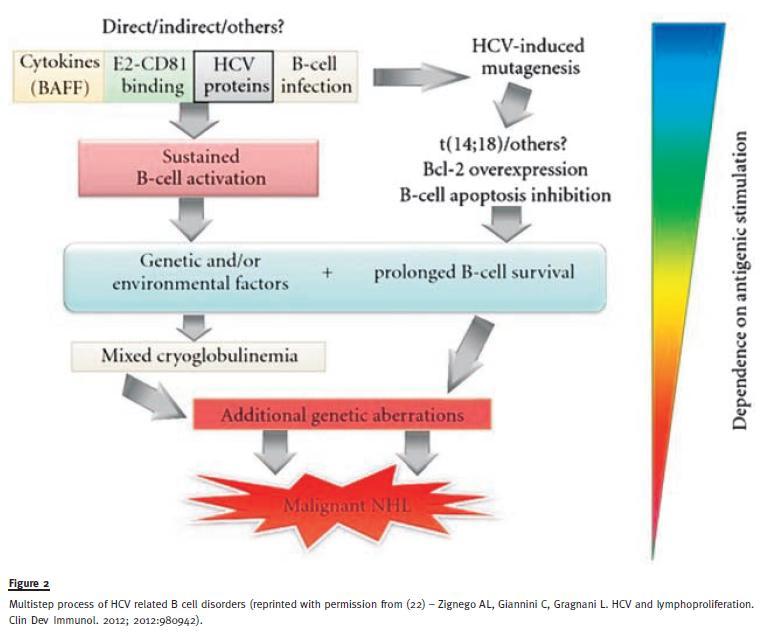
The exact mechanism linking HCV and the B cell is not perfectly understood. Several hypotheses, usually interconnected with each other, have been proposed (Fig.2)22. Main key factors seem to be the sustained HCV antigenic stimulation of the B cell compartment, chromosomal aberrations and immune mediators, such as cytokines and chemokines23-28.
The explanation for the seemingly autonomy of the B cell disease development from antigenic HCV stimulus, may be related with the prolonged survival and accumulation of potentially auto-reactive B cells, even after withdrawal of the inciting stimulus, as demonstrated by Visentini et al.29. These considerations are the rationale for the use of a B cell depletor, like rituximab, in the treatment of severe or relapsing MC disease. This approach seems effective and could be preferential when significant renal involvement coexists limiting the use of conventional antiviral therapy. In our case, although considered, the good response to glucocorticoids and the immediate unavailability of RTX precluded its use. However, it would be a reasonable choice in similar cases.
In conclusion, with this report, we emphasize the possibility of HCV related MC occurrence and its renal manifestations, in patients with sustained virus eradication.
Our discussion highlights the latest advances in the physiopathology understanding of HCV related B cell disorders and its implications on the therapeutic regimen choices.
References
1. Lauer G, Walker BD. Hepatitis C virus infection. N Engl J Med 2001;345(1):41-52 [ Links ]
2. Dammacco F, Lauletta G, Montrone M, Sansonno D. Mixed cryoglobulinemia: a model of virus-related disease in internal medicine. Dig Liver Dis 2007;39 (Suppl 1):S8-S12 [ Links ]
3. DAmico G, Colasanti G, Ferrario F, Sinico RA. Renal involvement in essential mixed cryoglobulinemia. Kidney Int 1989;35(4):1004-1014 [ Links ]
4. Frankel AH, Singer DR, Winearls CG, Evans DJ, Rees AJ, Pusey CD. Type II essential mixed cryoglobulinemia: Presentation, treatment and outcomes in 13 patients. Q J Med 1992;82(298):101-124 [ Links ]
5. Misiani R, Bellavita P, Fenili D, et al. Interferon-alpha 2a therapy in cryoglobulinemia associated with hepatitis C virus. N Engl J Med 1994;330(11):751-756 [ Links ]
6. Saadoun D, Resche-Rigon M, Thibault V, Piette JC, Cacoub P. Antiviral therapy for hepatitis C virus-associated mixed cryoglobulinemia vasculitis: a long-term followup study. Arthritis Rheum 2006;54(11): 3696-3704 [ Links ]
7. Ferri C, Cacoub P, Mazzaro C, et al. Treatment with rituximab in patients with mixed cryoglobulinemia syndrome: results of multicenter cohort study and review of the literature. Autoimmun Rev 2011;11(1):48-55 [ Links ]
8. De Vita S, Quartuccio L, Isola M, et al. A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis. Arthritis Rheum 2012;64(3):843-853 [ Links ]
9. Fabris M, Quartuccio L, Sacco S, et al. B-Lymphocyte stimulator (BLyS) up-regulation in mixed cryoglobulinemia syndrome and hepatitis-C virus infection. Rheumatology (Oxford) 2007;46(1);37-43 [ Links ]
10. Boonyapisit K, Katirji B. Severe exacerbation of hepatitis C-associated vasculitic neuropathy following treatment with interferon alpha: a case report and literature review. Muscle Nerve 2002;25(6):909-913 [ Links ]
11. Beauthien W, Mellinghoff HU, Kempis JV. Vasculitic complications of interferon-alpha treatment for chronic hepatitis C infection: case report and review of the literature. Clin Rheumatol 2005;24(5):507-515 [ Links ]
12. Levine JW, Gota C, Fessler BJ, Calabrese LH, Cooper SM. Persistent cryoglobulinemic vasculitis following successful treatment of hepatitis C virus. J Rheumatol 2005;32(6):1164-1167 [ Links ]
13. Landau DA, Saadoun D, Halfon P, et al.Relapse of hepatitis C virus-associated mixed cryoglobulinemia vasculitis in patients with sustained viral response. Arthritis Rheum 2008;58(2): 604-611 [ Links ]
14. Inman RD, The role of infection in chronic arthritis. J Rheumatol Suppl 1992;33:98-104 [ Links ]
15. Radkowski M, Gallegos-Orozco JF, Jablonska J, et al. Persistence of hepatitis C virus in patients successfully treated for chronic hepatitis C. Hepatology 2005;41(1):106–114 [ Links ]
16. Pham TN, MacParland SA, Mulrooney PM, Cooksley H, Naoumov NV, Michalak TI. Hepatitis C virus persistence after spontaneous or treatment-induced resolution of hepatitis C. J Virol 2004;78(11):5867–5874 [ Links ]
17. Quartuccio L, De Marchi G, Fabris M, De Vita S. Development of type II cryoglobulinaemic syndrome after effective and persistent hepatitis C virus eradication. Rheumathology (Oxford) 2007;46(2):367-368 [ Links ]
18. Zignego AL, Macchia D, Monti M, t al. Infection of peripheral mononuclear blood cells by hepatitis C virus. J Hepatol 1992;15(3):382–386
19. Gisbert JP, Garcia-Buey L, Pajares JM, Moreno-Otero R. Prevalence of hepatitis C virus infection in B-cell non-Hodgkins lymphoma: systematic review and meta-analysis. Gastroenterology 2003;125(6):1723–1732 [ Links ]
20. Monti G, Pioltelli P, Saccardo F, t al. Incidence and characteristics of non-Hodgkin lymphomas in a multicenter case file of patients with hepatitis C virus-related symptomatic mixed cryoglobulinemias. Arch Intern Med 2005;165(1):101–105
21. Gisbert JP, Garcia-Buey L, Pajares JM, Moreno-Otero R. Systematic review: regression of lymphoproliferative disorders after treatment for hepatitis C infection. Aliment Pharmacol Ther 2005;21(6): 653–662. [ Links ]
22. Zignego AL, Giannini C, Gragnani L. HCV and lymphoproliferation. Clin Dev Immunol 2012;2012:980942 [ Links ]
23. De Re V, Sansonno D, Simula MP, t al. HCV-NS3 and IgG-Fc crossreactive IgM in patients with type II mixed cryoglobulinemia and B-cell clonal proliferations. Leukemia 2006;20(6):1145–1154
24. Rosa D, Saletti G, De Gregorio E, t al. Activation of naive B lymphocytes via CD81, a pathogenetic mechanism for hepatitis C virus-associated B lymphocyte disorders. Proc Natl Acad Sci U S A. 2005;102(51):18544-18549
25. Machida K, Tsukiyama-Kohara K, Sekiguch S, et al. Hepatitis C virus and disrupted interferon signaling promote lymphoproliferation via type II CD95 and interleukins. Gastroenterology 2009;137(1):285-296 [ Links ]
26. Zignego AL, Ferri C, Giannelli F, t al. Prevalence of bcl-2 rearrangement in patients with hepatitis C virus-related mixed cryoglobulinemia with or without B-cell lymphomas. Ann Intern Med 2002;137(7):571-580
27. Giannini C, Giannelli F, Zignego AL. Association between mixed cryoglobulinemia, translocation (14;18), and persistence of occult HCV lymphoid infection after treatment. Hepatology 2006;43(5):1166–1167 [ Links ]
28. Sansonno D, Tucci FA, Troiani L, et al.Increased serum levels of the chemokine CXCL13 and up-regulation of its gene expression are distinctive features of HCV-related cryoglobulinemia and correlate with active cutaneous vasculitis, Blood 2008;112(5):1620–1627 [ Links ]
29. Visentini M, Conti V, Cagliuso M, t al. Persistence of a large population of exhausted monoclonal B cells in mixed cryoglobuliemia after the eradication of hepatitis C virus infection. J Clin Immunol 2012;32(4):729-735
Dr. Rui Andre Silva
Nephrology Department, Hospital do Espirito Santo
Largo Senhor da Pobreza
7000 – Evora, Portugal
E-mail: rui.a.silva.hevora@gmail.com
Acknowledgments
The authors gratefully acknowledge Dr. Fernanda Carvalho and Dr. Helena Viana for the kidney biopsy pictures (Department of Renal Morphology, Hospital Curry Cabral, Lisbon, Portugal).
Conflict of interest statement: None declared.
Received for publication: 19/07/2013
Accepted in revised form: 05/11/2013


{kind=link}
{kind=link}