










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.4 Lisboa dez. 2013
ORIGINAL ARTICLE
Clinical evolution in adults with nephrotic syndrome diagnosed in paediatric ages – a single-centre experience
Evolução clínica em adultos com síndroma nefrótica diagnosticada na idade pediátrica – experiência de um centro
Marta Neves1, Luis Escada1, Luis Rodrigues1, Clara Gomes2, Jorge Pratas1, Antonio Jorge Correia2, Mario Campos1
1Nephrology Department, Centro Hospitalar e Universitário de Coimbra. Coimbra, Portugal.
2Pediatric Nephrology Unit, Centro Hospitalar e Universitário de Coimbra. Coimbra, Portugal.
ABSTRACT
Background: Most renal disorders affecting children (apart from simple urinary infections) are chronic and the majority of these children require additional and specific nephrological care throughout adulthood, with undeniable physical, psychological and social implications arising therefrom. Aim: The primary aim of the current study was to examine the clinical outcome of patients suffering from nephrotic syndrome, transferred for continued care from a tertiary paediatric facility to the adult-oriented Nephrology Department at the Centro Hospitalar e Universitario de Coimbra. Subjects and Methods: Data collection was registry-based and retrospectively collected. General characterization of the 109 patients transferred is supplied, followed by an analysis of the 28 patients with a diagnosis of nephrotic syndrome. Clinical outcomes evaluated included need for ongoing immunosuppressive therapy, disease recurrence, progression to chronic kidney disease and/or renal replacement therapy, anaemia, phosphorus and calcium metabolism, serum albumin and proteinuria. Results: The two most prevalent groups of glomerular diseases presenting with nephritic syndrome were minimal change disease and focal and segmental glomerulosclerosis. Half of the patients with nephrotic syndrome are currently off chronic immunosuppressive therapy and disease recurrence occurred in only three of the 22 patients still followed at our Nephrology Department during the final year of follow-up (mean follow-up of 82.7 ± 59.7 months). Those who developed chronic kidney disease with need for renal replacement therapy had focal and segmental glomerulosclerosis on the initial kidney biopsy. Conclusions: Our results corroborate those found in other published studies and patients still followed remain clinically stable, with only three suffering disease relapse during the final year of follow-up. The specificities of kidney disorders diagnosed in childhood and their individual aspects deserve special care and benefit from a transition appointment involving the patient´s paediatrician and a nephrologist, as well as from the upkeep of national prospective registries dedicated to paediatric kidney disease.
Key-words: Immunosuppression; nephrotic syndrome; paediatric age.
RESUMO
Introdução: A maioria das alterações renais que afectam as crianças (excluindo as infecções urinárias simples) são crónicas, e a generalidade destas crianças necessita de cuidados nefrológicos específicos durante a vida adulta, com inegáveis implicações físicas, psicológicas e sociais daí decorrentes. Objectivos: O objectivo primário deste estudo foi avaliar a evolução clínica dos pacientes com síndroma nefrótica, transferidos de uma unidade pediátrica terciária, para continuação de cuidados no Serviço de Nefrologia do Centro Hospitalar e Universitário de Coimbra. Material e Métodos: A colheita de dados foi retrospectiva e baseada em registos hospitalares. É fornecida a caracterização geral dos 109 pacientes transferidos, seguido de uma análise dos 28 pacientes com diagnóstico de síndrome nefrótica. Os resultados clínicos avaliados incluíram a necessidade de terapêutica imunossupressora de manutenção, recorrência da doença, progressão para doença renal crónica e/ou terapêutica de substituição da função renal, anemia, fósforo e metabolismo do cálcio, albumina sérica e proteinúria. Resultados: Os dois grupos mais prevalentes de doenças glomerulares que se apresentaram com síndroma nefrótica foram a doença de lesões mínimas e a glomeruloesclerose focal e segmentar. Metade dos pacientes com síndroma nefrótica estão actualmente sem terapêutica imunossupressora e recorrência da doença de base ocorreu em apenas três dos 22 pacientes ainda em seguimento no nosso Serviço durante o último ano de seguimento (tempo médio de seguimento 82,7 ± 59,7 meses). Aqueles que desenvolveram doença renal crónica com necessidade de terapêutica de substituição da função renal apresentavam glomeruloesclerose focal e segmentar na biópsia renal inicial. Conclusões: Os nossos resultados corroboram os encontrados em outros estudos publicados e os que mantêm seguimento continuam clinicamente estáveis, com apenas três recidivas durante o último ano de seguimento. As especificidades das patologias renais diagnosticadas na infância e os seus aspectos particulares merecem atenção especial e beneficiariam de uma consulta de transição que envolvesse o pediatra do paciente e um nefrologista, bem como a manutenção de registos nacionais dedicados à doença renal pediátrica.
Palavras-chave: Idade pediátrica; imunossupressão; síndroma nefrótica.
INTRODUCTION
Most renal disorders affecting children (other than simple urinary tract infections) are chronic and the majority of these children require additional and specific nephrological care throughout adulthood1.
It is important to realize that not only are their renal diseases somewhat different from the remaining adult population, but their expectations (and those of their parents) towards their illness and towards the subsequent follow-up throughout their adult life are probably also different. The transition process should be individualized for each patient, communication should be enhanced and all aspects of physical and psychological development should be addressed2. Although the management of those with an evident requirement of continued care remains vital, it is unclear which of the apparently well patients with nephrological pathologies, such as Henoch-Schonlein purpura, haemolytic uraemic syndrome or previous episodes of acute kidney injury, require referral to an adult nephrology facility. The need for evidence-based guidelines for their subsequent management is, therefore, manifest3. Idiopathic nephrotic syndrome is the most common form of childhood nephrotic syndrome and this diagnosis represents an important motive for referral to adult nephrology facilities. It is imperative to understand that nephrotic conditions diagnosed during childhood are somewhat different from those diagnosed in adulthood, and to recognise the implications that may arise from these chronic disorders, particularly regarding patient expectations during follow-up (even after being in remission for many years) and the anticipated clinical evolution during the adult age. The primary aim of the current study was to examine the clinical outcome of patients suffering from nephritic syndrome (those whose diagnosis at the time of transfer was primary nephrotic syndrome and those transferred with a diagnosis of chronic kidney disease (CKD) secondary to nephrotic conditions), transferred for continued care from a tertiary paediatric facility to the adult-oriented Nephrology Department at the Centro Hospitalar e Universitario de Coimbra.
SUBJECTS AND METHODS
We retrospectively studied patients transferred between the 1st January 1996 and 30th June 2012 from Coimbra´s Paediatric Hospital and followed for at least 6 months or until initiation of renal replacement therapy (RRT) at the Nephrology Department of the Centro Hospitalar e Universitario de Coimbra.
Patients transferred to the Nephrology Department were those referred by the paediatric nephrologist for kidney disease requiring ongoing care (supervision or specific treatment) throughout adulthood. Before 2011, this referral was made when children were between the age of fifteen and sixteen. Children referred for kidney transplantation were transferred at any age and those in which it was predicted that dialysis would be needed in the short term were transferred from the age of ten. As of January 2011, children with kidney disease remained in the care of the paediatrician until they reached the age of 18 and were later transferred. The transition is prepared in advance by the patients paediatric nephrologist, who explains the reasons for this to the patient and the parents. Currently, at our Nephrology Department, patients are randomly assigned to a nephrologist for regular consultations. The patients then have one additional follow-up appointment with the paediatric nephrologist in order to address any remaining doubts or concerns. Once a nephrologist has been assigned, the patient remains in his/her care at the Centro Hospitalar e Universitario de Coimbra until loss to followup, referral to extra-hospital haemodialysis units, peritoneal dialysis, transplantation or death.
Data collection was registry-based and 109 patients were included in the analysis. Characterization and general description of these patients is supplied, concerning demographic data and diagnoses at transfer to the Nephrology Department.
This descriptive analysis is followed by a more in-depth investigation of patients with nephritic syndrome. The 28 patients with nephrotic syndrome in this analysis include those with a primary and secondary diagnosis of nephrotic syndrome i.e., those whose diagnosis at the time of transfer was primary nephrotic syndrome (n = 23) and those transferred with a primary diagnosis of CKD secondary to glomerular diseases presenting or coursing with nephritic syndrome (n = 5).
We collected demographic data, laboratory data (serum creatinine, blood urea nitrogen (BUN), haemoglobin, serum calcium, serum phosphate, parathyroid hormone (PTH) level, serum albumin and 24-hour proteinuria), presence of obesity at transfer (defined as body mass index at or above the 95th per presence of hypertension at transfer (defined as average systolic blood pressure and/or diastolic blood pressure that is greater than or equal to the 95th percentile for sex, age, and height on three or more occasions in patients ≤ 18 years) and immunosuppressive medication instituted during follow-up. Estimated Glomerular Filtration Rate (eGFR) was calculated by using the Modification of Diet in Renal Disease (MDRD) formula4 in patients over the age of 18 and by the revised Schwartz formula5 in children.
Data was gathered at the time of transfer, at regular intervals after transfer (six months, one year, two years and five years) and at the final evaluation.
For statistical purposes, only data at the time of transfer and at final evaluation were analysed and, consequently, presented. Clinical outcomes that were evaluated included need for ongoing immunosuppressive therapy, disease recurrence, progression to CKD and/or RRT, anaemia, phosphorus and calcium metabolism, serum albumin and proteinuria. All statistical calculations were performed using the commercially available software program SPSSR (version 17.0, SPSS, Chicago, IL, USA) for WindowsR.
Continuous variables are presented as means ± standard deviation, and categorical variables as a percentage of the number of studied cases. Comparisons between unrelated quantitative variables were performed using the t test or the Mann Whitney U test; related quantitative variables were performed using the paired t test; and nominal variables were compared by using the χ2 test. P values < 0.05 are reported as statistically significant.
RESULTS
One hundred and nine patients met the inclusion criteria: 68 males (62.4%) and 41 females (37.6%).
Mean age at diagnosis of renal pathology was 5.1 ± 4.4 years (54.1% were below the age of five at that time) and they were followed at the Paediatric Nephrology Unit for 119.2 ± 61.8 months. Mean age at the time of transfer was 15.0 ±3.0 years. The predominant diagnoses at transfer were CKD (stage 3 to 5 in 30 patients – 27.5%, stage 5 requiring need for RRT in 15 patients – 13.8%), nephrotic syndrome (21.1%, n = 23), tubulopathies (11.9%, n = 13, four of which (30.8%) due to hypophosphatemic rickets), urinary sediment anomalies with no specific diagnosis (6.4%, n = 7), reflux nephropathy (4.6%, n = 5), lupus nephritis (2.8%, n = 3), IgA nephropathy (2.8%, n = 3), autosomal dominant polycystic kidney disease (1.8%, n = 2) and other renal disorders in the remaining eight patients.
Nephrotic Syndrome
The 28 patients in this analysis include those whose diagnosis at the time of transfer was primary nephrotic syndrome and those transferred with a diagnosis of CKD secondary to nephrotic conditions.
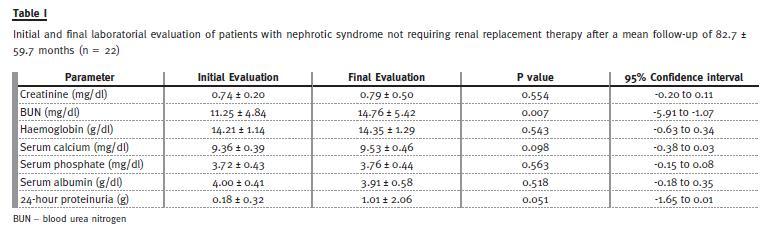
The majority of the patients with nephrotic syndromewere males (67.9%, n = 19), glomerular disease was diagnosed at the mean age of 5.8 ± 2.9 years and they were followed at the Paediatric Nephrology Unit for a mean time of 119.6 ± 39.6 months. Mean age at the time of transfer was 15.7 ± 1.7 years, 10.7% of patients presented below the fifth percentile with regard to weight and 28.6% below the fifth percentile concerning height, with obesity being present in 21.4% of cases. Only two patients had arterial hypertension (7.1%). Twenty-two patients (78.6%) were submitted to renal biopsy: minimal change disease was diagnosed in 15 children (53.6%), six of which had some degree of mesangial proliferation, focal and segmental glomerulosclerosis (FSGS) was diagnosed in six children (21.4%) and one patient had membranous nephropathy (3.6%). During followup at the Paediatric Nephrology Unit, corticosteroids were employed in all patients (corticodependence in 71.4% and corticoresistance in 10.7%), with a need for, at least, one cycle of treatment with oral cyclophosphamide in 19 patients (67.9%) – 11 of these required two cycles of treatment with the alkylating agent. Cyclosporin A was the therapeutic agent of choice as third-line therapy in eight patients (28.6%) and levamisole in two patients. Mean follow-up as outpatients at the adult Nephrology Department was 82.7 ± 59.7 months. Seven patients progressed to stage 3 to 5 CKD – one with an eGFR of 27 ml/ min/1.73m2 on final evaluation (no histopathological diagnosis, corticodependent) and six patients required RRT – all with FSGS on the initial kidney biopsy. In this population of patients, obesity and hypertension were not risk factors for the progression to CKD (both with p= 0.99). The treatment of choice in the first RRT was haemodialysis in three patients, peritoneal dialysis in two patients and pre-emptive live donor kidney transplantation in one patient. Twentytwo patients (78.6%) maintain regular follow-up at the Nephrology Department, half of them (54.5%) with no need for current immunosuppressive medication (half of these were patients that required secondor third-line immunosuppressive agents sometime during follow-up to induce clinical remission of the nephrotic syndrome). Maintenance dose corticosteroids are still required in ten patients (five of which in association with cyclosporin A). Only three patients (13.6%) had one or more episode of recurring nephrosis in the final year of follow-up. The laboratory data at initial and final evaluation at the Nephrology Department of those patients with nephritic syndrome not requiring RRT (n = 22) are presented in Table I.
DISCUSSION
Idiopathic nephrotic syndrome is the most common form of childhood nephrotic syndrome, representing more than 90% of cases between the age of one and ten years and 50% of cases above the age of ten6, which is concordant with the mean age at diagnosis of nephrotic syndrome in our population (5.8 ± 2.9 years). The International Study of Kidney Disease in Children has also reported a majority of patients with histologic findings of minimal change disease7, present in more than half of the patients in our studied population, with the vast majority responding to an empirical course of steroid therapy, permitting deferral of kidney biopsies, according to subsequent clinical course. Initial studies reported a prevalence of FSGS of 7%6, but subsequent studies have demonstrated an increasing prevalence of FSGS8,9, which may have implications in the future management of nephrotic syndrome in children. Treatment-resistant forms of idiopathic nephrotic syndrome can result in progressive CKD10 and, based on the North American Pediatric Renal Trials and Collaborative Studies (NAPRTCS) 2011 annual report, FSGS is the third most common primary renal disease in the transplant cohort and the most prevalent group in the dialysis registry (11.7% and 14.4%, respectively)11.
In conclusion, the two most prevalent groups of kidney disorders at our department were glomerular diseases presenting with nephrotic syndrome (minimal change disease in 53.6% and FSGS in 21.4%) and CKD. Half of the patients with nephrotic syndrome are currently off chronic immunosuppressive therapy and disease recurrence occurred in only three of the 22 patients still followed at our Nephrology Department during the final year of follow-up. No statistical differences were found between the initial and final laboratory evaluation of these patients with regard to haemoglobin, calcium, phosphate and albumin levels. Their kidney function also remained stable (initial creatinine 0.74 ± 0.20 vs. 0.79 ± 0.50 mg/dl at final evaluation, p = 0.554). Statistically, BUN increased significantly from 11.25 ± 4.84 to 14.76 ± 5.42 mg/dl (p = 0.007), although remaining within normal laboratory values and, therefore, not considered clinically significant. Although not statistically significant (p = 0.051), 24-hour proteinuria was higher at final evaluation (0.18 ± 0.32 vs. 1.01 ± 2.06 g), reflecting the elevated proteinuria arising from the three patients who relapsed during that final year of follow-up. By eliminating these three patients from the analysis, 24-hour proteinuria was 0.12 ± 0.24 g at initial evaluation and 0.44 ± 1.13 g at the final evaluation (p = 0.192). The population of patients with nephrotic syndrome who developed CKD with need for RRT had FSGS on the initial kidney biopsy.
An interesting future analysis would be to look at the long-term adverse effects associated with the use of chronic immunosuppression in these patients, regarding incidence of osteoporosis, cataracts, glucose intolerance or malignancies. Further studies are required to prospectively analyse lasting remission rates, particularly of steroid-resistant forms of nephritic syndrome diagnosed in childhood and followed during adulthood.
Limitations to this study include its retrospective and single-centre nature, which can be a source of bias and confound, restricted by the quantity (and quality) of data in the records, not permitting generalization of the results obtained. In hindsight, data on stature growth, dyslipidaemia, glucose intolerance, cognitive function and school performance throughout follow-up would allow for additional and interesting analyses that could have a further impact on current clinical practice.
The specificities of kidney illnesses diagnosed in childhood and their particular (and sometimes unfamiliar) aspects, which may represent a continuing constant throughout adulthood, deserve special attention. Patients benefit from a specific joint transition appointment involving the patient´s paediatrician and a nephrologist who can devote care to this area12, in addition to other health professionals, including dieticians and psychologists (who may be helpful in addressing issues such as non-compliance), contemplating a multidisciplinary approach to these patients.
References
1. Cameron JS. The rocky road of transition from paediatric to adult care in renal disease. Port J Nephrol Hypert 2007;21(3):185-186. [ Links ]
2. Watson AR. Problems and pitfalls of transition from paediatric to adult renal care. Pediatr Nephrol 2005;20(2):113-117. [ Links ]
3. Cameron JS. The continued care of children with renal disease into adult life. Pediatr Nephrol 2001;16(8):680-685. [ Links ]
4. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999;130(6):461-470. [ Links ]
5. Schwartz GJ, Munoz A, Schneider MF, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol 2009;20(3):629-637. [ Links ]
6. ISKDC. Nephrotic syndrome in children: prediction of histopathology from clinical and laboratory characteristics at time of diagnosis. A report of the International Study of Kidney Disease in Children. Kidney Int 1978;13(2):159-165. [ Links ]
7. ISKDC. The primary nephrotic syndrome in children. Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the International Study of Kidney Disease in Children. J Pediatr 1981;98(4)561-564. [ Links ]
8. Filler G, Young E, Geier P, Carpenter B, Drukker A, Feber J. Is there really an increase in non-minimal change nephrotic syndrome in children? Am J Kidney Dis 2003;42(6):1107-1113. [ Links ]
9. Bonilla-Felix M, Parra C, Dajani T, t al. Changing patterns in the histopathology of idiopathic nephrotic syndrome in children. Kidney Int 1999;55(5):1885-1890.
10. ISKDC. Primary nephrotic syndrome in children: clinical significance of histopathologic variants of minimal change and of diffuse mesangial hypercellularity. A Report of the International Study of Kidney Disease in Children. Kidney Int 1981;20(6):765–771. [ Links ]
11. NAPRTCS: 2011 Annual Report. Available at https://web.emmes.com/study/ped/announce.htm. (accessed on March 17, 2013). [ Links ]
12. Jorge S, Neves FC, Mendonca E, Stone R, Almeida M, Martins Prata M. Paediatric nephrology patients moving to adult age: a difficult transition to manage. The experience of a paediatric-to-adult out-patient clinic. Port J Nephrol Hypert 2007;21(3):211-217. [ Links ]
Dra Marta Neves
Nephrology Department,
Centro Hospitalar e Universitario de Coimbra
Praceta Professor Mota Pinto
3000-075 Coimbra, Portugal
E-mail: martaraq_neves@hotmail.com
Conflict of interest statement: None declared.
Received for publication: 02/07/2013 Accepted in revised form: 25/11/2013


{kind=link}