










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.3 Lisboa set. 2013
Unusual bacteria causing peritonitis in peritoneal dialysis – A single centre experience
Bactérias raras como causa de peritonite em diálise peritoneal – A experiência de um centro
Ana Farinha, Alvaro Vaz, Jose Assuncao, Jose Vinhas
Department of Nephrology, Centro Hospitalar de Setúbal, Setúbal, Portugal
ABSTRACT
Background:Peritonitis is one of the most common complications of peritoneal dialysis. The most frequent agents have been largely described and studied but unusual microorganisms have only been reported in case reports. Methods: We describe the cases of unusual bacteria causing peritonitis in our peritoneal dialysis patients between 1998 and 2012. Results: In this 15-year period, we have registered 188 peritonitis in 118 patients (0.64 episodes/patient/year). Unusual bacteria were considered all that have caused peritonitis in only one or two instances (12 bacteria in 15 episodes). We have performed antibiogram-based antibiotic therapy in all of them. In two cases catheter removal was necessary and one patient has died in direct relation with the peritonitis. Conclusions: Unusual bacterial agents may cause peritonitis in peritoneal dialysis. They are rare and may present with a broad spectrum of seriousness. Publication of experiences may help guiding therapy and increases scientific evidence.
Key-words: Peritoneal dialysis; Peritonitis; Unusual bacteria
RESUMO
Introdução: A peritonite e uma das complicações mais comuns em dialise peritoneal. Os agentes mais frequentes têm sido amplamente descritos e estudados, mas os agentes raros apenas o tem sido em case reports. Métodos: Descrevemos a casuística de bactérias raras que causaram peritonite nos doentes em dialise peritoneal (DP) da nossa Unidade de 1998 a 2012. Resultado: Neste período de 15 anos, registamos 188 peritonites em 118 doentes (0,64 episódios/doente/ano). Foram consideradas bactérias raras todas as que causaram peritonites em um ou dois episódios (12 bactérias em 15 peritonites). A antibioterapia foi baseada no teste de sensibilidade antibiótica de cada microorganismo. Em dois casos foi necessário remover o cateter e noutro caso o paciente morreu em relação directa com a peritonite. Conclusões: Algumas bactérias raras podem causar peritonites em doentes em DP. Estas peritonites são pouco frequentes e podem apresentar uma grande diversidade na sua evolução. A apresentação de experiencias aumenta a evidencia e pode ajudar a orientar o tratamento destas situações.
Palavras-chave: Bactérias pouco frequentes, Dialise Peritoneal, Peritonite
INTRODUCTION
Peritonitis is one of the most frequent complications in peritoneal dialysis and remains one of the most important causes for patient dropout1. Grampositives are the most frequent microorganisms responsible for peritonitis2. Advances in connectology led to a significant decline in the incidence of Gram-positive infections, but new pathogens emerged3.
When an unusual agent is present it may be difficult to answer some questions, such as how pathogenic is this agent, how long antibiotics should be prescribed or if the catheter should be removed. Previous case reports may help to guide therapeutic decisions, so we report our single centre experience.
RESULTS
Our Unit has followed 118 patients, between 1998 and 2012. Their mean age was 57.7 ± 14.7 years and most were male (53.4%). The end-stage renal disease (ESRD) aetiology was diabetes mellitus nephropathy in 30% of cases, chronic glomerulonephritis in 17%, chronic interstitial nephritis in 11%, polycystic disease in 8%, hypertensive nephroangiosclerosis in 7% and in 24% of the cases it was unknown. The mean time in peritoneal dialysis (PD) was 2.5 years. Most of our patients (66%) have been on continuous ambulatory peritoneal dialysis (CAPD) and the remaining were on APD.
We have witnessed a changing pattern in most common agents causing peritonitis in this 15-year period. We registered 188 peritonitis in 118 patients (0.64 episodes/patient/year). Gram-positive were responsible for most peritonitis (50%) but there has been a decrease in Staphylococcus aureus incidence from 1.39 episodes/patient/year to 0.1 episodes/patient/year . Gram-negatives were responsible for 21.8% of all peritonitis. Escherichia coli, Pseudomonas aeruginosa and Enterobacteriacae were the most frequent Gram-negative agents isolated. Mixed infections occurred in 3.2% of the cases and fungi in 2.7%. In 22.3% of the peritonitis no agent has been isolated in effluent cultures.
Our protocol of empirical antibiotherapy has also changed. Between 1998 and 2002, patients diagnosed with peritonitis were treated empirically with intraperitoneal (IP) vancomycin and netilmicin. Since 2002, all patients were treated with intraperitoneal vancomycin and ceftazidime.
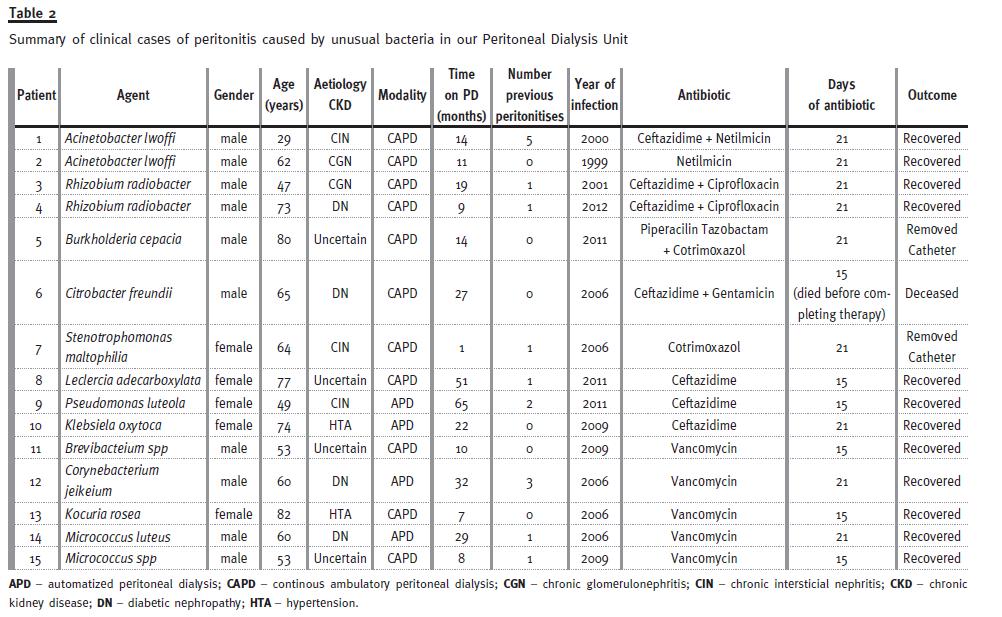
Occasionally, we have seen peritonitis by unusual microorganisms. The agents that have caused peritonitis in only one or two instances were considered as unusual (Table I). Our objective was to describe peritonitis caused by unusual bacteria in our peritoneal dialysis patients and to review the microbiology of these agents. Their clinical situations are summarized in Table II.
ACINETOBACTER LWOFFI
Acinetobacterspecies are aerobic Gram-negative bacilli that occur in pairs. They are non-fermentative, oxidase-negative and non-motile bacteria (from where its name derives, akinetic)4. They can survive on moist and dry surfaces being mainly soil organisms.
They can also be found in hospital environments where they may be a source of infection in debilitated patients5. Acinetobacter lwoffi peritonitis in PD patients has rarely been reported6. Acinetobacter are innately resistant to many classes of antibiotics, including penicillin, chloramphenicol, and often aminoglycosides. Resistance to fluoroquinolones has also been reported. Carbapenems are recognized as the gold-standard treatment7, nevertheless, Acinetobacter lwoffi(formerly Mima Polymorpha) seems to be more susceptible to antibiotics4.
In our Unit we have registered the following two cases:
Patient 1. A 62-year-old male on CAPD for 11 months presented for the first time with abdominal pain and cloudy effluent for 24 hours. The white blood cell count (WBCC) of dialysis fluid showed 3500 WBC/mm3, 90% of neutrophils. A. lwoffi was isolated. It was resistant to cephalosporins but sensitive to aminoglycosides. He took 21 days of IP netilmicin with a good response.
Patient 2. A 29-year-old male on CAPD for 14 months was admitted to our hospital complaining of abdominal pain and vomiting for 24 hours. A peritoneal dialysis exchange was performed, showing cloudy effluent (1900 WBC/mm3). His evolution to a septic state forced him to stay in-hospital for 6 days. A. lwoffi was isolated and it was resistant to first generation cephalosporins. He was successfully treated with netilmicin and ceftazidime.
RHIZOBIUM RADIOBACTER
Rhizobium(formerly agrobacterium) species are aerobic Gram-negative motile bacillus. They are mainly soil organisms. Occasionally, they have been associated with human infections especially in immunocompromised patients with indwelling catheters8. In PD patients, a few cases of Rhizobium peritonitis have been reported 9-13. The outcome seems to be favourable when antibiogram-based therapy is used.
Prolonged treatment (21 days)12,13 has been associated to better outcome obviating the need for catheter removal9. Paucity of data does not allow establishing an antibiotic resistance profile.
We have registered two cases of Rhizobium radiobacter peritonitis with more than a decade apart.
Patient 1. A 47-year-old male on CAPD presented to the PD Unit with abdominal pain. He denied cloudy effluent, but when an exchange was made, cytological examination showed 3278 WBC/mm3, predominantly neutrophils. Rhizobium radiobacter was identified with a resistance pattern to aminoglycosides. He was medicated with ceftazidime IP for 21 days, but 3 days after completing therapy he presented cloudy effluent again. On this occasion, no agent was found, but, assuming the same aetiology, 15 days of IP ciprofloxacin was prescribed according to the previous antibiogram. The same patient presented a third peritonitis but a Gram+ was identified and a new antibiotic course of vancomycin and amikacin was administered for 21 days. Fortunately, he recovered completely and remained on CAPD for one more year peritonitisfree.
Patient 2. A 73-year-old male on CAPD went to the hospital because of abdominal pain and cloudy effluent. When asked, he recalled an exchange with a damaged dialysis bag. The effluent presented 5000 WBC/mm3, mainly neutrophils. IP ceftazidime was prescribed with good initial response. However, because of the previous patient evolution, we decided to add ciprofloxacin per os when Rhizobium radiobacter was isolated. He recovered completely. No other peritonitis was registered.
BURKHOLDERIA CEPACIA
Burkholderia cepacia is an aerobic Gram-negative bacillus. It is found in human skin as commensal.
It may cause pneumonia in immunocompromised patients with underlying lung disease, such as cystic fibrosis or chronic granulomatous disease14. It has been rarely associated with peritonitis in PD15 and it is naturally resistant to many common antibiotics, such as aminoglycosides and polymyxin B.
Treatment typically requires an antibiotic association that should include some of the following ceftazidime, doxycycline, piperacillin, meropenem, chloramphenicol and trimethoprim/sulfamethoxazole(cotrimoxazole)16.
Our patient was an 80-year-old male, immunocompromised because of prostatic cancer. He was medicated with DecapeptylR and ZometaR. He had history of a Proteus mirabilis exit-site infection, 5 months earlier, but without any previous peritonitis.
He presented with abdominal pain, vomiting and cloudy effluent. The cell count of peritoneal fluid was 5200 WBC/mm3 with neutrophil predominance (90%). He was empirically medicated following our protocol (vancomycin + gentamicin). Six days later, the peritoneal microbiology was known and the antibiogram showed resistance to aminoglycosides and cephalosporins. The evolution was ominous, so it was decided to keep the patient hospitalized to remove the catheter. A change in antibiotics was done and IV piperacillin-tazobactam and co-trimoxazole per os were initiated. The patient was transferred to haemodialysis.
CITROBACTER FREUNDII
Citrobacter freundii is a facultative anaerobic Gramnegative bacillus. It can be found in soil, water, sewage, food and the intestinal tract of animals and humans. It is classified under the Enterobacteriaceaes family17. As an opportunistic pathogen, C. freundii is responsible for a number of significant opportunistic infections. It is known to cause nosocomial infections of the respiratory tract, urinary tract, blood and many other normally sterile sites18. A few Citrobacter freundii peritonitis in PD have been reported19,20. Various patterns of resistance have been described because of extended-spectrum B-lactamase (ESBL)19,20.
Our patient was a 65-year-old diabetic male, with multiple micro and macrovascular complications. He was admitted to our hospital in a septic status. He complained of abdominal pain. The effluent cell count showed 2670 WBC/mm3, with 87% polymorphonuclear (PMN). Empiric antibiotherapy was initiated.
When Gram stain was known (Gram-negative) an abdominal ultrasonography and a CT scan were performed to exclude abdominal complications. Citrobacter freundii was isolated and it was resistant to penicillins and first-generation cephalosporins. The antibiotics were changed to ceftazidime and gentamicin following the antibiogram, but the patient maintained cloudy effluent and abdominal pain.
Therefore, IV piperacillin-tazobactam was initiated.
The patient died before the scheduled catheter removal.
STENOTROPHOMONAS MALTOPHILIA
Stenotrophomonas maltophilia is an aerobic, nonfermentative Gram-negative bacterium. Initially classified as Pseudomonas maltophilia, S. maltophilia was also grouped in the genus Xanthomonas and, finally, in the genus Stenotrophomonas, in 1993.
Stenotrophomonas maltophilia is catalase and oxidase-negative (distinguishing it from other members)21. It is ubiquitous in aqueous environments, soil and plants22. It is not a virulent organism but may be associated to infected prosthesis that may be necessary to remove, like PD catheters. Peritonitis in PD patients with this agent have been reported with and without catheter infection23-26. Stenotrophomonas. maltophiliais naturally resistant to many broad-spectrum antibiotics (including carbapenems), due to the production of β-lactamases 16. Sensitivity testing requires non-standard culture techniques with incubation at 30 °C27. Testing at the wrong temperature results in isolates being incorrectly reported as being susceptible when they are, in fact, resistant.
Many strains of S. maltophilia are sensitive to cotrimoxazole and ticarcillin, although resistance has been increasing28. It is not usually susceptible to piperacillin, and susceptibility to ceftazidime is variable29.
We report a 64-year old woman, who presented peritonitis to Pseudomonas aeuroginosa 10 days after initiating CAPD. After antibiogram was known, she was medicated with ceftazidime and gentamicin but, 10 days later, she complained once more of abdominal pain. The effluent cell count showed 5000 WBC/mm3 90% PMN, so it was decided to remove the catheter immediately. Stenotrophomonas maltophilia was isolated in the peritoneal effluent and in the removed catheter. By that time, antimicrobial sensitivity pattern was known and the patient was treated for 21 days with cotrimoxazol. She was switched to haemodialysis.
LECLERCIA ADECARBOXYLATA
Leclercia adecarboxylata is a facultative anaerobic Gram-negative bacillus. It is classified under the Enterobacteriaceaes family and formerly known as Escherichia adecarboxylata. It is the unique of its genus. Its pathogeny is uncertain and it rarely causes human infection30. Only two cases have been reported in the literature, as far as we know31. The antibiotic of the bacillus is unknown.
A 77-year old woman was admitted to our PD Unit for abdominal pain and cloudy dialysate. The WBCC on dialysate showed 6000/mm3, 80% PMN.
Empiric antibiotherapy was initiated with vancomycin and ceftazidime IP. When L. adecarboxylata was isolated, ceftazidime IP was maintained for 15 days and the patient presented an excellent recovery.
PSEUDOMONAS LUTEOLA
Pseudomonas luteola is an aerobic, non-fermentative Gram-negative bacillus. In 1987, it was moved to the genus Chryseomonas luteola, but returned again to Pseudomonas genus in 199732. It is a soil and water saprophyte but it has been rarely associated with cellulitis and bacteraemia33. Pseudomonas luteola peritonitis in PD has been described previously in one case34.
Resistance profiles have been described to amoxicillin, first generation cephalosporin and co-trimoxazole35.
We present a 49-year old woman, with CKD due to staghorn calculi. She had two previous peritonitis to Pseudomonas putida, the first two years before and another, one year before. These peritonitis were respectively treated with ceftazidime for 21 days and with ciprofloxacin plus gentamicin for 21 days. She presented a third time with fever (37.8 oC), abdominal pain and cloudy peritoneal dialysate (29.100 WBC/mm3, 90% PMN). On this occasion, Pseudomonas luteola was identified and the evolution with IP ceftazidime was uneventful.
KLEBSIELA OXYTOCA
Klebsiela oxytoca is a facultative anaerobic Gramnegative bacillus from the Enterobacteriaceae´s family.
It is recognized as a rare human pathogen. To our knowledge, there is only one case of peritonitis in PD caused by Klebsiela oxytoca and it was a mixed infection with Pseudomonas aeuriginosa36.
No resistances have been reported.
A 74-year old woman was admitted to our PD 48 hours. The dialysate was cloudy and 17500 WBC/mm3, 90% PMN were identified. She initiated vancomycin and ceftazidime. When she was re-evaluated 48 hours later, she was completely asymptomatic.
Klebsiela oxytoca was isolated, vancomycin was stopped and the peritonitis cured.
BREVIBACTERIUM SPECIES
Brevibacterium is a Gram-positive bacillus. Some species are found in cheese. Brevibacterium casei and Brevibacterium epidermidis are found in human skin and are responsible for odour. Sometimes it is responsible for infections, particularly associated with prosthesis37. A few cases of peritonitis have been described in PD patients38. Resistance to β-lactamics, ciprofloxacin, clindamycine and erythromycin where described and it is sensitive to gentamicin, rifampicin and tetracycline.
A 53-year-old male on CAPD was admitted because of cloudy dialysate and abdominal pain.
The WBCC showed 585 WBC/mm3, 85% PMN. A Brevibacterium spp was identified and it was sensitive to all tested antibiotics. He was treated with vancomycin with an excellent evolution: in 24 hours he was asymptomatic.
MICROCOCCUS SPECIES
Micrococcus is an obligate aerobe Gram-positive coccus that typically appears in tetrads. Micrococcus occurs in a wide range of environments, including water, dust, and soil. Micrococcus is generally thought to be a saprophytic or commensal organism, although it can be an opportunistic pathogen, particularly in immunocompromised patients, such as those with HIV39. It can be difficult to identify Micrococcus as the cause of an infection, since the organism is normally present in skin microflora, and the genus is seldom linked to disease, but recurrent bacteremia, septic shock, septic arthritis, endocarditis, meningitis, and cavitating pneumonia have been reported. A few cases of peritonitis have also been described40. Micrococcus luteus colonizes the mammalian skin. Moreover, the bacterium colonizes the human mouth, mucosae, oropharynx and upper respiratory tract. To exclude Staphylococcus aureus, a bacitracin susceptibility test can be performed41.
We had at our Unit two cases of Micrococcus peritonitis:
Patient 1. A 60-year-old diabetic male with advanced retinopathy that seriously compromised his vision, had been on APD for 2 years. He was admitted to our Unit due to accidental disconnection of the cycler lines during the treatment. An exchange with dwell time of 2 hours was done to obtain a dialysate sample. The WBCC showed 880 WBC/mm3, 80% PMN and, therefore, empiric IP antibiotics were administered. A M. luteus was isolated and the patient was kept on vancomycin therapy for 21 days on APD with excellent evolution.
Patient 2. The same patient that presented a Brevibacterium peritonitis, was readmitted three months latter for cloudy effluent. He denied abdominal pain, as he denied any problem with the PD technique. The WBCC revealed 1900/mm3 with 90% PMN. A Micrococcus was isolated. The species was not identified. Vancomycin was maintained for 15 days and the patient remained free from peritonitis for the following 3 years.
CORYNEBACTERIUM JEIKEIUM
Corynebacterium jeikeium is an aerobic Grampositive bacillus. It is pathogenic, typically causing an opportunistic infection, seen most frequently in bone marrow transplant patients but a few cases in PD have been reported42-43. It is usually susceptible to vancomycin and tetracycline. Resistance to macrolide antibiotics is common44.
Our patient that previously developed M. luteus peritonitis was admitted two months later with abdominal pain. The WBCC obtained from dialysate showed 3900/mm3, 80% PMN. By that time no risk factor has been identified. Corynebacterium jeikeium was isolated and the patient was successfully treated with vancomycin for 21 days. Like in other unusual Gram-positive peritonitis, the evolution was excellent.
The patient was kept in APD at his request.
KOCURIA ROSEA
Kocuria rosea is an aerobic, gram-positive coccus. It is found in tetrads, irregular clusters or cubical packets of eight. It was previously classified into the genus Micrococcus. This organism is widespread in nature and is frequently found as normal skin flora in humans and other mammals. In this genus, the majority of strains are non-pathogenic, but Kocuria rosea may be opportunistic.
It has been reported to cause catheter-related bacteraemia41 and peritonitis45-46. Apart from nitrofurantoin, no other resistances have been reported47.
An 82-year-old woman was admitted to our hospital because of severe abdominal pain and cloudy peritoneal dialysate for 5 hours. The WBCC in effluent showed > 16000/mm3, > 95% PMN. A K. rosea was isolated a few days later. Contrasting with the severity of presentation, after two dwells with empiric antibiotic the patient was asymptomatic. She took 15 days of IP vancomycin with complete recovery.
DISCUSSION
In 15 years we have registered 15 peritonitis due to unusual bacterial agents in 12 patients (0.05 episodes/patient/year). Twelve patients recovered completely without need for catheter removal, but in two cases (Burkholderia cepacia and Stenotrophomonas maltophilia) there was a need to drop-out of haemodialysis, and one patient died in direct relation to his peritonitis (Citrobacter freundii).
The International Society of Peritoneal Dialysis (ISPD) infection guidelines advise to deliver antibiotic therapy according to the resistance pattern (possibly with 2 drugs) for 14-21 days, if a clinical response is seen, but the catheter must be removed if no clinical improvement is achieved within 5 days48.
In our protocol, we do 2 weeks of antibiotic for most common bacterial peritonitis and 3 weeks for Staphylococcus aureus, Pseudomonas species, Xantomonas species and other Gram-negatives. In general, Gram-negative peritonitis precludes longer treatments, because they usually have worse prognosis.
We applied that principle to our Gram-negative peritonitis presented here, so we do not know if shorter regimens could be effective.
Until enough data about unusual bacteria peritonitis exists, it is wise to individualize treatment and monitor the response to treatment. Catheter removal should be proposed if the organism is multi-resistant or if the clinical situation deteriorates.
In our opinion, a national PD registry would help us defining what is uncommon, how to treat unusual peritonitis depending on patterns of resistance and what to expect from each of those rare situations.
The therapeutic strategy for rare peritonitis agents in PD can be improved with new published experiences.
References
1. Fried LF, Bernardini J, Johnston JR, Piraino B. Peritonitis influences mortality in peritoneal dialysis patients. J Am Soc Nephrol 1996;7:2176-2182 [ Links ]
2. Piraino B, Bernardini J, Sorkin M. A five-year study of the microbiologic results of exit site infections and peritonitis in continuous ambulatory peritoneal dialysis. Am J Kidney Dis 1987; 10:281–286. [ Links ]
3. Port FK, Held PJ, Nolph KD, Turenne MN, Wolfe RA. Risk of peritonitis and technique failure by CAPD connection technique: a national study. Kidney Int. 1992;42(4):967-974. [ Links ]
4. Gerner-Smidt P, Frederiksen W. Acinetobacter in Denmark: I. Taxonomy, antibiotic susceptibility, and pathogenicity of 112 clinical strains. APMIS 1993; 101(11):815-825 [ Links ]
5. Visca P, Seifert H, Towner KJ. Acinetobacter infection–an emerging threat to human health. IUBMB Life 2011;63(12):1048-1054 [ Links ]
6. Huddam B, Kocak G, Azak A, Duranay M. Acinetobacter lwoffii peritonitis in a patient receiving continuous ambulatory peritoneal dialysis. Ther Apher Dial 2013;17(1):117-119. [ Links ]
7. Rahal JJ. Novel antibiotic combinations against infections with almost completely resistant Pseudomonas aeruginosa and Acinetobacter species. Clin Infect Dis 2006; 43 (Suppl 2): S95-99 [ Links ]
8. Lai CC, Teng LJ, Hsueh PR, et al. Clinical and microbiological characteristics of Rhizobium radiobacter infections. Clin Infect Dis 2004;38(1):149-153 [ Links ]
9. Han KH, Han SY. A Case of Rhizobium Radiobacter Peritonitis Cured without Removal of the PD Catheter in a Patient on CAPD. Korean J Nephrol 2007;26:634-636 [ Links ]
10. Rodby RA, Glick EJ. Agrobacterium radiobacter peritonitis in two patients maintained on chronic peritoneal dialysis. Am J Kidney Dis 1991;18(3):402-405 [ Links ]
11. Rothe H, Rothenpieler U. Peritonitis due to multiresistant rhizobium radiobacter. Perit Dial Int 2007;27(2):214–215 [ Links ]
12. Minguela JI, de-Pablos M, Castellanos T, Ruiz-de-Gauna R. Peritonitis by Rhizobium radiobacter. Perit Dial Int 2006:26(1):112 [ Links ]
13. Marta R, Damaso C, Silva JE, Almeida M. Peritonitis due to Rhizobium radiobacter. Einstein 2011; 9:389-390 [ Links ]
14. Mahenthiralingam E, Urban TA, Goldberg JB. The multifarious, multireplicon Burkholderia cepacia complex. Nat Rev Microbiol 2005;3(2):144–156. [ Links ]
15. Kang HM, Park JE, Lee HD, et al. A case of Burkholderia cepacia peritonitis in a patient on CAPD. Korean J Med 2006;7:219-223 [ Links ]
16. McGowan JE Jr. Resistance in nonfermenting gram-negative bacteria: multidrug resistance to the maximum. Am J Infect Control 2006;34(5 Suppl 1): S29–37;S64–73 [ Links ]
17. Wang JT, Chang SC, Chen YC, Luh KT. Comparison of antimicrobial susceptibility of Citrobacter freundii isolates in two different time periods. J Microbiol Immunol Infect 2000;33(4):258–262 [ Links ]
18. Whalen JG, Mully TW, English JC 3rd. Spontaneous Citrobacter freundii infection in an immunocompetent patient. Arch Dermatol 2007;143(1): 124–125 [ Links ]
19. Gursu M, Aydin Z, Pehlivanoglu F, et al. Citrobacter peritonitis: two cases and review of the literature. Perit Dial Int 2011;31(4):409-411 [ Links ]
20. Dervisoglu E, Yumuk Z, Yegenaga I. Citrobacter freundii peritonitis an tunnel infection in a patient on continuous ambulatory peritoneal dialysis. J Med Microbiol 2008; 57(1):125-127 [ Links ]
21. Palleroni N, Bradbury JF. Stenotrophomonas, a new bacterial genus for Xanthomonas maltophilia (Hugh 1980) Swings et al. 1983. Int J Syst Bacteriol 1993;43(3): 606–609 [ Links ]
22. Denton M, Kerr KG. Microbiological and clinical aspects of infection associated with Stenotrophomonas maltophilia. Clin Microbiol Rev 1998;11(1):57–80 [ Links ]
23. Azak A, Kocak G, Huddam B, Scan G, Duranay M. An unusual cause of continuous ambulatory peritoneal dialysis–associated outpatient peritonitis: Stenotrophomonas maltophilia. Am J Infect Control 2011;39(7):618 [ Links ]
24. Taylor G, McKenzie M, Buchanan-Chell M, Perry D, Chui L, Dasgupta M. Peritonitis due to Stenotrophomonas maltophilia in patients undergoing chronic peritoneal dialysis. Perit Dial Int 1999;19(3):259-262 [ Links ]
25. Tzanetou K, Triantaphillis G, Tsoutsos D, et al. Stenotrophomonas maltophilia peritonitis in CAPD patients: susceptibility to antibiotics and treatment outcome: a report of five cases. Perit Dial Int 2004;24:401-404 [ Links ]
26. Baek JE, Jung EY, Kim HJ et. al Stenotrophomonas maltophilia infection in patients receiving continuous ambulatory peritoneal dialysis. Korean J Intern Med 2004;19:104-108 [ Links ]
27. Wheat PF, Winstanley TG, Spencer RC. Effect of temperature of antimicrobial susceptibilities of Pseudomonas maltophilia. J Clin Pathol 1985; 38(9):1055–1058. [ Links ]
28. Pankuch GA, Jacobs MR, Applebaum PC. Susceptibilities of 123 Xanthomonas maltophilia strains to clinafloxacin, PD131628, PD138312, PD140248, ciprofloxacin, and ofloxacin. Antimicrob Agents Chemother 1994;38(2): 369–370 [ Links ]
29. Pankuch GA, Jacobs MR, Rittenhouse SF, Appelbaum PC. Susceptibilities of 123 strains of Xanthomonas maltophilia to eight beta-lactams (including beta-lactam-beta-lactamase inhibitor combinations) and ciprofloxacin tested by five methods. Antimicrob Agents Chemother 1994;38(10):2317–2322. [ Links ]
30. Hess B, Burchett A, Huntington MK. Leclercia adecarboxylata in an immunocompetent patient. J Med Microbiol 2008;57:896–898 [ Links ]
31. Fattal O, Deville JG. Leclercia adecarboxylata peritonitis in a child receiving chronic peritoneal dialysis. Pediatr Nephrol 2000;15(3-4):186-187. [ Links ]
32. Casalta JP, Fournier PE, Habib J, Riberi A, Raoult D. Prosthetic valve endocarditis caused by Pseudomonas luteola. BMC Infect Dis 2005;5:82 [ Links ]
33. Arnold FW, Sciortino CV, Riede KA. New Associations With Pseudomonas Luteola Bacteremia: A Veteran With A History Of Tick Bites And A Trauma Patient With Pneumonia. The Internet Journal of Infectious Diseases. 2005:4 [ Links ]
34. Amber IJ, Reimer LG. Pseudomonas sp. group Ve-2 bacterial peritonitis in a patient on continuous ambulatory peritoneal dialysis. J Clin Microbiol 1987;25(4):744-745 [ Links ]
35. Chihab W, Alaoui AS, Amar M. Chryseomonas luteola identified as the source of serious infections in a Moroccan University Hospital. J Clin Microbiol 2004;42(4):1837–1839 [ Links ]
36. Yang SB, Yang WC, Chen TW, Lin CC. Klebsiella oxytoca and polymicrobial infection in peritoneal dialysis-related peritonitis. Perit Dial Int 2004;24(2):196-197 [ Links ]
37. Ulrich S, Zbinden R, Pagano M, Fischler M, Speich R. Central venous catheter infection with Brevibacterium sp. in an immunocompetent woman: case report and review of the literature. Infection 2006;34(2):103-106 [ Links ]
38. Choi JS, Kim CS, Park JW, ET AL. Consecutive episodes of peritonitis in a patient undergoing peritoneal dialysis caused by unusual organisms: Brevibacterium and Pantoea agglomerans. Kidney Res Clin Pract 2012; 31:121–123 [ Links ]
39. Smith KJ, Neafie R, Yeager J, Skelton HG. Micrococcus folliculitis in HIV-1 disease. Br J Dermatol 1999;141(3):558–561 [ Links ]
40. Kao CC, Chiang CK, Huang JW. Micrococcus species-related peritonitis in patients receiving peritoneal dialysis. Int Urol Nephrol 2012 Oct 9. [Epub ahead of print] [ Links ]
41. Schiffl H, Lang S. Non-diphtheria corynebacteria and CAPD infections. Nephrol Dial Transplant 2009; 24(12):3896-3897 [ Links ]
42. Szeto CC, Chow KM, Chung KY, Kwan BC, Leung CB, Li PK. The clinical course of peritoneal dialysis-related peritonitis caused by Corynebacterium species. Nephrol Dial Transplant 2005;20(12):2793–2796 [ Links ]
43. Rosato AE, Lee BS, Nash KA. Inducible macrolide resistance in Corynebacterium jeikeium. Antimicrob Agents Chemother 2001;45(7):1982–1989 [ Links ]
44. Altuntas F, Yildiz O, Eser B, Gundogan K, Sumerkan B, Cetin M. Catheter-related bacteremia due to Kocuria rosea in a patient undergoing peripheral blood stem cell transplantation. BMC Infect Dis 2004;4(1):62. [ Links ]
45. Dotis J, Printza N, Papachristou F. Peritonitis attributable to Kocuria rosea in a pediatric peritoneal dialysis patient. Perit Dial Int 2012;32(5):577-578. [ Links ]
46. Kaya KE, Kurto ğlu Y, Cesur S, et al. Peritonitis due to Kocuria rosea in a continuous ambulatory peritoneal dialysis case. Mikrobiyol Bul 2009;43(2):335-337 [ Links ]
47. Savini V, Catavitello C, Masciarelli G, et al. Drug sensitivity and clinical impact of members of the genus Kocuria. J Med Microbiol 2010;59(Pt12):1395–1402. [ Links ]
48. Li PK, Szeto CC, Piraino B, et al. Peritoneal dialysis-related infections recommendations: 2010 update. Perit Dial Int 2010;30(4):393-423 [ Links ]
Dra Ana Farinha
Av. D. Joao II, no12, 7oDto,
2910-548 Setubal, Portugal
E-mail: alpfarinha@yahoo.com.br
Conflicts of interest statement: None declared
Received for publication: 04/04/2012
Accepted in revised form: 18/07/2013


{kind=link}
{kind=link}