










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.2 Lisboa abr. 2013
Visceral leishmaniasis: an unexpected diagnosis during the evaluation of pancytopenia in a kidney transplant recipient
Leishmaniose visceral: um diagnóstico inesperado na avaliação de uma pancitopenia num doente transplantado renal
Pêgo C1,2, Romãozinho C1,2, Santos L1,2, Macário F1,2, Alves R1,2, Campos M1, Mota A2
1 Department of Nephrology
2 Renal Transplantation Unit and Department of Urology
Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
ABSTRACT
The aetiological study of cytopenia in solid organ transplant recipients could be challenging, given the need to exclude infectious disorders, drug toxicity or neoplastic disease. Visceral leishmaniasis is endemic in several regions of the world, but a rare complication after renal transplantation (less than 100 cases described in literature).
We report the case of a male renal transplant recipient, 57 years of age, admitted to our Unit 17 months after transplantation with febrile illness and severe pancytopenia. He had a history of leucopenia and thrombocytopenia detected in follow-up exams two months earlier, with progressive worsening despite discontinuation of drugs with potential haematologic toxicity. On admission, his complaints were weakness, night sweats and weight loss. On examination, he was febrile, pale, and had a palpable spleen. Laboratory exams demonstrated: leukocytes 1.1 x109/L, platelets 68 x109/L, haemoglobin 10.3 g/dl, serum creatinine 1.48 mg/dl, C-reactive protein 9.72 mg/dl. Abdominal ultrasound confirmed splenomegaly. A bone marrow aspiration was performed and antibiotic therapy was instituted empirically, without improvement. Additional laboratory results were inconclusive: negative blood and urine cultures, no evidence of cytomegalovirus, parvovirus B19 or HIV infections, hepatitis B and C and masses/ adenopathies were excluded by computerized tomography. Despite the absence of an evident epidemiological context, the bone marrow examination showed amastigotes of Leishmania spp. He was started on liposomal amphotericin B (4 mg/kg/day; total of 10 administrations) with a sustained clinical and laboratory improvement after the second day of therapy.
Visceral leishmaniasis is a potentially lethal infection if treatment is delayed or not instituted. Although rare among renal transplant recipients it should be included in the differential diagnosis of febrile pancytopenia.
Key-Words: Kidney transplantation; liposomal amphotericin B; pancytopenia; visceral leishmaniasis
RESUMO
O estudo etiológico das citopenias nos doentes submetidos a transplante de órgãos sólidos constitui um desafio dada a multiplicidade de causas subjacentes: infeções, toxicidade medular induzida por fármacos ou doença hematológica. A leishmaniose visceral (LV) é uma doença endémica em diversas regiões do globo, sendo, contudo, uma complicação rara após a transplantação renal (TR) (menos de 100 casos descritos na literatura).
Os autores descrevem o caso de um doente do sexo masculino, 57 anos, transplantado renal, internado na unidade de TR 17 meses após o transplante por síndrome febril e pancitopenia grave. O doente apresentava leucopenia e trombocitopenia com 2 meses de evolução e de agravamento progressivo, apesar da suspensão da terapêutica potencialmente mielotóxica e queixas de astenia, sudorese nocturna e perda ponderal. Ao exame objectivo encontrava-se febril, com palidez muco-cutânea e esplenomegalia. O estudo laboratorial inicial revelou leucócitos 1,1 x109/l, plaquetas 68 x109/l, hemoglobina 10,3 g/dl, creatinina 1,48 mg/dl e proteína C reactiva 9,72 mg/dl e a ecografia abdominal confirmou a existência de esplenomegalia.
Realizada punção aspirativa de medula óssea e iniciada terapêutica antibiótica empírica sem melhoria clínica.
O estudo analítico adicional foi inconclusivo: culturas de sangue e de urina negativas, sem evidência de infeção por citomegalovírus, parvovírus B 19, VIH, vírus da hepatite B ou C. Excluídas massas tumorais e adenopatias por tomografia computorizada. Apesar da inexistência de um contexto epidemiológico óbvio, o exame de medula óssea revelou presença de amastigotas de Leishmania spp. Iniciada anfotericina B lipossómica (4 mg/Kg/dia; total de 10 administrações) com registo de melhoria clínica e laboratorial a partir do 2º dia de tratamento. A LV é uma infeção potencialmente fatal se o tratamento adequado não for instituído/iniciado tardiamente. Apesar de constituir uma complicação infeciosa rara após a TR, os autores destacam a importância da sua inclusão no diagnóstico diferencial de pancitopenia febril neste grupo de doentes.
Palavras-chave: Anfotericina B lipossómica; leishmaniose visceral; pancitopenia; transplantação renal.
INTRODUCTION
In solid organ transplant recipients cytopenias frequently occur during the first months post-transplantation.
Drug toxicity and infectious disorders (mostly viral) are the major causes, with primary haematologic disease being less common, but aetiological diagnosis could be challenging1. The two main causes of post-transplant infection are the reactivation of latent infection (donor tissue/recipient origin) and the acquisition of new microorganisms from the community or hospital2. Pre-transplant evaluation with detailed exposure history and laboratory tests are essential to prevent post-transplant infection and/or for an early and specific diagnosis in cases where prophylactic or pre-emptive therapies are not indicated.
Besides the general screening profile – human immunodeficiency virus (HIV) 1 and 2, hepatitis B and C virus (HBV/HCV), cytomegalovirus (CMV), Epstein-Barr virus (EBV) and tuberculosis –, selected patients should be screened for specific occult infections, depending on the past exposure to endemic infections3.
Leishmaniasis is an endemic parasitic infection in several regions of the globe caused by the protozoan of the genus Leishmania. Visceral leishmaniasis (VL) in Mediterranean and Middle Eastern countries and Brazil is due to Leishmania infantum, and the transmission of the parasite is mainly zoonotic from the domestic dog (major reservoir) to humans by sand fly vector (genus Phlebothomus in Europe)4,5. There are also other forms of parasite transmission, like organ transplantation, intravenous drug use, blood transfusion or laboratory contamination, but these modes of transmission are rare6-9. In Portugal, the disease is endemic in three geographic areas (Alto Douro, Lisbon and Tagus Valley and the Algarve), although cases have been reported throughout the country10,11.
Visceral leishmaniasis due to L. infantum most commonly affects children and HIV patients and, less frequently, organ transplant recipients. Clinical manifestations of VL usually include non-specific symptoms and signs like malaise, fever and weight loss, which have a slow progression of weeks or months12.
Laboratory findings most frequently include leucopenia, anaemia, thrombocytopenia, with pancitopoenia in a significant number of patients10,12. Hypergammaglobulinaemia could be present and results from polyclonal B-cell activation. Radiologic exams show splenomegaly in approximately 70% of cases and hepatomegaly in 60% in some series10. Definitive diagnosis requires the identification of the parasite by smear or culture in affected tissue, usually bone marrow. Despite being a rare complication after transplantation (less than 100 cases reported in the literature), the kidney is the most affected organ (77% of cases)7. If appropriate treatment is delayed or not instituted, VL is a life-threatening condition13.
Liposomal amphotericin B (LAB) is the drug with the highest therapeutic efficacy and the lowest toxicity profile14,15.
CASE REPORT
We report the case of a 57-year-old male, renal transplant recipient, who was admitted to our Hospital 17 months after renal transplantation (March 2012) with fever and severe pancytopenia. He had a history of leucopenia and thrombocytopenia detected in follow-up laboratory exams two months earlier, with progressive worsening despite gradual reduction of mycophenolic acid and discontinuation of other drugs with potential haematologic toxicity.
On admission, the patient referred complaints of malaise, weakness, night sweats and a 7Kg weight loss in the previous month. On physical examination, he was pale, febrile (39 °C), normotensive and had a palpable spleen. The remaining examination was normal: normal cardiac and pulmonary auscultations, no signs of meningeal irritation and no lymphadenopathies.
He was medicated with tacrolimus LP 2mg id, prednisolone 5mg id, omeprazol 20mg id, amlodipine 10mg id, carvedilol 12,5mg bid.
The patients past medical history included chronic renal disease of unknown aetiology, hypertension and hyperuricaemia. In October 2010, he received a kidney transplant from a deceased donor. The allograft had immediate function and there were no medical or surgical complications in the post-transplantation period. During follow-up as a renal transplant recipient, and until January 2012, he had no intercurrences and his basal serum creatinine was 0.8 mg/dl. He had no contact with pets or other animals, no occupational or recreational exposures and denied high-risk behaviours. He had always lived in Águeda – Portugal, and had vacationed in Brazil and Thailand ten years earlier.
Laboratory studies on admission showed the following results: white blood cells (WBC) 1.1 x109/L (4-10 x109/L), platelets 68 x109/L (150-400 x109/L), red blood cells (RBC) 3.68x1012/L (4.5-5.5 x1012/L), haemoglobin 10.3 g/dl (13-17 g/dl), serum creatinine 1.48 mg/dl (0.72-1.18 mg/dl), normal ionogram, PCR 9.72 mg/dl (0-0.5 mg/dl), normal liver function and coagulations tests. Abdominal ultrasonography detected a homogeneous enlarged spleen of 17 cm in length and a normal liver. On admission, antibiotic therapy was started empirically (ceftazidime), and on the 1st day of hospitalization he started granulocyte-colony stimulating factor due to the worsening leucopenia (WBC 0.8 x109/L) and valganciclovir due to suspected CMV infection. In order to exclude a haematologic aetiology we requested evaluation by a haematologist, and on the 2nd day of hospitalization bone marrow aspiration was performed.
The complementary laboratory study later came to reveal: negative blood and urine cultures; negative CMV antigenemia and viral load; no serological evidence of active infection by CMV, EBV, B19 parvovirus, HBV, HCV or HIV; negative blood and urine BK polyoma virus viral load; normal folic acid and B12 vitamin; serum iron 27 ug/dl (70-180 ug/dl), transferrin saturation 15% (20-40%) and ferritin 4366 ng/ml (20-250 ng/ml). The CT scan of the chest, abdomen and pelvis showed no changes other than splenomegaly. On the 7th day, he was still febrile and there was no significant improvement in the laboratory findings (WBC 2.3 x 109/L).
On the 8th day of hospitalization, and despite the absence of a clear epidemiological context, the results from the bone marrow examination revealed the presence of extracellular amastigotes of Leishmania spp. The detection of anti-Leishmania antibodies was subsequently requested and was positive (direct immunofluorescence and Western blot).
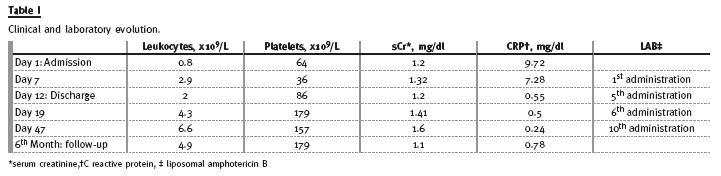
With a definitive diagnosis of VL, the patient was started on LAB intravenously and ceftazidime was suspended. After 2 days of therapy, he became afebrile and pancytopenia started to improve in a sustained way. The therapeutic regimen included a total of 10 LAB administrations in a dose of 4 mg/Kg/day: 5 daily doses plus 5 weekly administrations (at the 10th, 17th, 24th, 31st and 38th days). After the 5th administration the patient was clinically stable and was discharged. The remaining LAB doses were administered on an outpatient basis. Before the 6th LAB administration (one week after the 5th dose) the laboratory exams showed a complete recovery of cytopenias (Table I). However, on physical examination the patient had purpuric skin lesions on the lower limbs and lower abdominal region.
He had no other complaints, including fever or arthralgia, and coagulation tests were normal. He was re-admitted for vigilance and the 6th LAB administration consisted in half the standard dose. The cutaneous lesions had gradually reverted and he was discharged 2 days later. During the treatment with LAB, the patient developed the following laboratory abnormalities: mild but progressive increase in serum creatinine (maximum value of 1.6 mg/dl) (Table I), hypocalcaemia and hypokalemia. The electrolyte disturbances were corrected with intravenous replacement therapy and resolved after discontinuation of the drug.
In this case, the treatment of VL with LAB was effective and well tolerated, despite the mild and transient adverse effects. During the six-month followup period there was no evidence of clinical or laboratory relapse (Table I). Due to the long-term risk of recurrence, the patient was also scheduled for outpatient follow-up by the Infectious Diseases department.
DISCUSSION
To our knowledge, this is the first case of VL in a renal transplant recipient reported in Portugal. In our patient, there was no evidence of high-risk exposure to Leishmania spp because he had never lived in geographic areas where the disease is endemic.
However, there are reports of VL in non-transplant recipients from non-endemic areas of our country10,11 and the patients travel history included a short stay in Brazil (an endemic area of VL). The transplanted organ as a source of infection is a more remote hypothesis, but was also a possibility (donors epidemiological history was not known).
After hospital admission, the multidisciplinary approach was crucial for prompt diagnosis and treatment since all studies were inconclusive until the identification of the parasite in the bone marrow aspirate. LAB is the most effective agent for VL treatment and, when compared to the previous amphotericin B formulations, shows less global toxicity including nephrotoxicity. However, treatment with LAB is associated with decline of the glomerular filtration rate induced by vasoconstriction and with direct tubular injury, which is responsible for disorders like hypokalaemia, renal tubular acidosis and hypercalciuria. In our patient, LAB treatment was associated with a progressive serum creatinine increase, asymptomatic hypocalcaemia (secondary to hypercalciuria) and hypokalaemia, but all adverse effects were completely reversed after drug discontinuation (Table I). During treatment, our patient also developed a purpuric rash. The cutaneous manifestations appeared between the 5th and 6th LAB administration and was probably secondary to LAB, since the platelet count was already normal at that time. LAB infusion-related dermatologic adverse reactions have been reported and consist mainly in pruritus/ urticaria16. The development of other cutaneous manifestations during the LAB treatment is very rare17.
Despite being a rare infectious complication after transplantation, VL most frequently affects kidney transplant recipients and, therefore, should be considered in the differential diagnosis of fever and/or pancytopenia, particularly in patients who reside or travel to areas where the disease is endemic. After VL diagnosis, successful treatment surveillance is critical since most patients harbour viable parasites lifelong and disease can recur18,19.
References
1. Viglietti D, Peraldi MN. Cytopenias following kidney transplantation. Nephrol Ther 2011;7(6):474-478 [ Links ]
2. Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med 2007; 357(25):2601-2614 [ Links ]
3. Avery RK, Recipient screening prior to solid-organ transplantation. Clin Infect Dis 2002;35(12):1513-1519 [ Links ]
4. Control of the leishmaniases. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser 1990;793:1-158 [ Links ]
5. Bern C, Maguire JH, Alvar J. Complexities of assessing the disease burden attributable to leishmaniasis. PLoS Negl Trop Dis 2008;2(10):e313. [ Links ]
6. Dey A, Singh S. Transfusion transmitted leishmaniasis: a case report and review of literature. Indian J Med Microbiol 2006; 24(3):165-170 [ Links ]
7. Antinori S, Cascio A, Parravicini C, Bianchi R, Corbellino M. Leishmaniasis among organ transplant recipients. Lancet Infect Dis 2008;8(3):191-199 [ Links ]
8. Herwaldt BL, Juranek DD. Laboratory-acquired malaria, leishmaniasis, trypanosomiasis, and toxoplasmosis. Am J Trop Med Hyg 1993;48(3):313-323. [ Links ]
9. Cruz I, Morales MA, Noguer I, Rodriguez A, Alvar J. Leishmania in discarded syringes from intravenous drug users. Lancet 2002; 359(9312):1124-1125 [ Links ]
10. Serrada EG, Leishmaniose visceral em Portugal continental (1999-2009) [dissertation]. Lisboa: Universidade Nova de Lisboa; 2010. Available from: http://hdl.handlenet/10362/5546 [ Links ]
11. Campino L, Maia C. Epidemiologia das leishmanioses em Portugal, Acta Med Port 2010;23(5):859-864 [ Links ]
12. Jeronimo SMB, de Queiroz Sousa A, Pearson RD. Leishmaniasis. In: Guerrant RL, Walker DH, Weller PF, editors. Tropical infectious diseases: principles, pathogens and practice. 2nd ed. Edinburgh, Scotland: Churchill Livingstone Elsevier; 2006. p.1095-1113 [ Links ]
13. Veroux M, Corona D, Giuffrida G, et al. Visceral leishmaniasis in the early post-transplant period after kidney transplantation: clinical features and therapeutic management, Transpl Infect Dis 2010;12(5):387-391 [ Links ]
14. Bern C, Adler-Moore J, Berenguer J, et al. Liposomal amphotericin B for the treatment of visceral leishmaniasis. Clin Infect Dis 2006;43(7):917-924 [ Links ]
15. Sundar S, Mehta H, Suresh AV, Singh SP, Rai M, Murray HW.Amphotericin B treatment for Indian visceral leishmaniasis: conventional versus lipid formulations. Clin Infect Dis 2004; 38(3):377-383 [ Links ]
16. Roden MM, Nelson LD, Knudsen TA, et al. Triad of acute infusion-related reactions associated with liposomal amphotericin B: analysis of clinical and epidemiological characteristics. Clin Infect Dis 2003;36(10):1213-1220 [ Links ]
17. Cagatay AA, Taranoglu O, Alpay N, et al. Amphotericin B-induced cutaneous leucocytoclastic vasculitis: case report. Mycoses 2008; 51(1): 81-82 [ Links ]
18. Bogdan C. Mechanisms and consequences of persistence of intracellular pathogens: leishmaniasis as an example. Cell Microbiol 2008;10(6):1221-1234 [ Links ]
19. de Rossel RA, de Duran RJ, Russel O Rodriguez AM. Is leishmaniasis ever cured? Trans R Soc Trop Med Hyg 1992;86(3):251-253 [ Links ]
Cátia Pêgo
Nephrology Department, Centro Hospitalar Tondela-Viseu
Avenida Rei D. Duarte 3504-509 VISEU-PORTUGAL
E-mail: catiapego@gmail.com
Conflict of interest statement. None declared.
Received for publication: 10/01/2013
Accepted in revised form: 17/05/2013


{kind=link}