










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.2 Lisboa abr. 2013
Emphysematous pyelonephritis complicating pauci-immune crescentic glomerulonephritis: a case report
Mubarak M, Manzoor K, Kazi JI, Hussain M
Histopathology, Nephrology and Urology Departments
Sindh Institute of Urology and Transplantation
Karachi, Pakistan
ABSTRACT
Emphysematous pyelonephritis is a rare, life-threatening condition, characterized by the presence of gas within the renal parenchyma, collecting system or perinephric tissue. It results from an acute severe necrotizing infection of the renal parenchyma, mostly in diabetic patients. We herein describe a young, male patient presenting with acute renal failure with a biopsy diagnosis of pauci-immune crescentic glomerulonephritis.
The patient was given steroids and immunosuppressants and discharged home with follow-up appointments. He presented again within one week with fever and right flank pain. Plain computed tomography abdomen revealed emphysematous pyelonephritis and right nephrectomy was performed along with administration of antibiotics and antifungals, but he died three days after surgery. Histopathological examination of the nephrectomy specimen showed extensive infarction, gas-filled cystic spaces and mucormycosis.
To our knowledge, this unique combination of kidney pathologies has not been reported in the literature before.
Key words: Acute renal failure, crescentic glomerulonephritis, diabetes mellitus, emphysematous pyelonephritis, mucormycosis
Implication for health policy/practice/research/medical education: Emphysematous pyelonephritis is a rare, life-threatening condition of the kidney and its collecting system characterized by acute necrotizing inflammation and gas formation. Its rapid and accurate diagnosis is of the utmost importance in instituting optimal treatment and preventing the high mortality. Prognosis of the condition has improved in recent years. A high index of suspicion coupled with appropriate investigations is the key for successful management of the condition.
INTRODUCTION
Emphysematous pyelonephritis (EPN) has been defined as an acute, severe, necrotizing infection of the renal parenchyma and perirenal tissue, which results in the presence of gas within the renal parenchyma, collecting system or perinephric tissue. Kelly and MacCallum reported the first case of EPN in 18981. Since then, many case reports and small series from single institutions have been published2-6. Literature search did not reveal a single published report of the entity from Pakistan. We herein present the first case report of the condition from this country and discuss the diagnostic and management issues of the case.
CASE REPORT
An 18-year-old male patient presented to Sindh Institute of Urology and Transplantation (SIUT) emergency department with the complaint of sore throat and pedal oedema for one month, productive cough with fever on and off for two weeks, and skin eruptions over face and feet for 10 days and occasional haemoptysis. Fever was gradual at onset, high-grade, intermittent, without rigors, associated with productive cough with yellow sputum and blood streaks.
There was no history of joint pain, haematuria, body swelling or shortness of breath. Past medical history was negative for hypertension, diabetes mellitus (DM), tuberculosis, stone disease or jaundice. Family history was unremarkable.
Laboratory investigations done at outside hospital showed haemoglobin 7.7 g/dl, white blood cells (WBCs) 9700/cmm, platelets 340,000/cmm, erythrocyte sedimentation rate (ESR) 102 mm/1st hour and urea/creatinine165/3 mg/dl, respectively. He was managed at outside hospital with intravenous fluids, steroids, antibiotics and blood transfusion and was subsequently transferred to SIUT.
Physical examination showed a young male of average height and built who was fully conscious and oriented in no acute distress. His vitals showed temperature of 100 0F, blood pressure 100/70 mmHg, and heart rate 92 beats/minute. General physical examination showed positive anaemia with a nonblanching, erythematous, maculopapular rash over both upper and lower limbs. The remaining physical examination did not reveal any abnormalities.
Laboratory investigations at SIUT showed haemoglobin of 7.8, haematocrit of 24, WBC count 9.6, and platelet count 389,000 per cmm. Urinalysis showed 2 + proteins, 3 + blood, numerous red blood cells (RBCs) and no pus cells. Biochemistry showed urea 210 mg/dl, creatinine 5.4 mg/dl, sodium 137 mEq/I, calcium 8.8 mg/dl, phosphorous 6.1 mg/dl, potassium 3.2 mEq/I, chloride 97 mEq/I, bicarbonate 20 mEq/I, total proteins 7.7 g/I, albumin 2.8 g/l, globulins 4.9 g/l, and albumin/globulin (A/G) ratio of 0.6. Ultrasound imaging showed normal size, non-hydronephrotic kidneys and chest X-ray (CXR) was unremarkable.
He was admitted with the diagnosis of acute renal failure (ARF) due to acute glomerulonephritis, and haemodialysis was performed because of worsening renal function. Culture tests due to fever, were negative and complete serology revealed negative antinuclear antibodies (ANA), anti-double stranded DNA antibody, hepatitis B surface antigen, hepatitis C antibodies, rheumatoid factor with normal complements.
A renal biopsy was performed, which showed single core of renal tissue with up to 18 glomeruli. Of these, 13 (72%) showed cellular crescents, the rest showing minor changes. There was patchy interstitial inflammation and acute tubular injury. Immunoflourescence examination showed trace positivity of IgM, C3 and C1q, while IgG and IgA were negative.
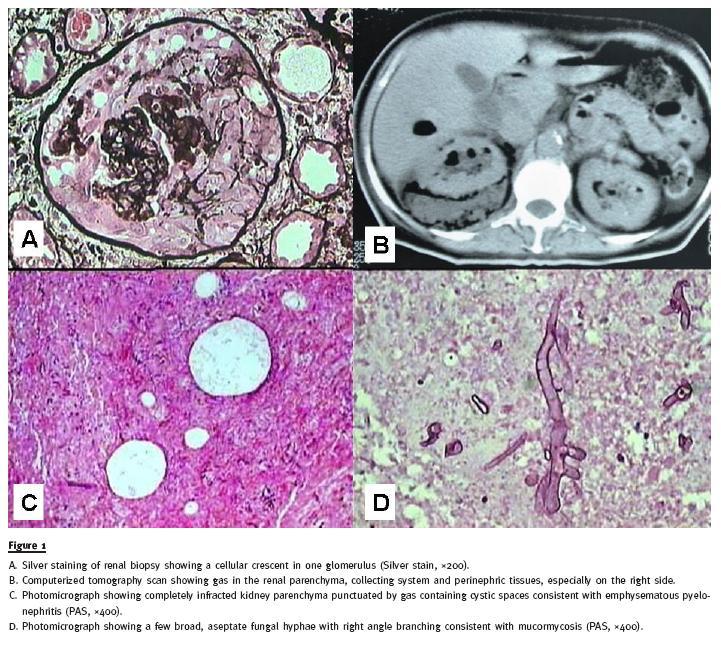
A final diagnosis of pauci-immune crescentic glomerulonephritis (Fig.1A) was made and the patient was started on pulse methyl prednisolone for three doses, followed by oral prednisolone, and one pulse of cyclophosphamide was given. He remained dialysis dependent with minimal urine output and was discharged one month after admission on oral prednisolone plus next dialysis appointment.
The patient was readmitted a week later with a one-day history of low-grade fever without rigors associated with non-radiating right flank pain, dull in nature. There were no other associated symptoms.
His examination showed a conscious and well-oriented male with cushingoid facies in no acute distress.
His vitals showed temperature of 99 0F, blood pressure of 110 / 70 mmHg and heart rate of 92 beats/minute. His general physical examination showed positive anaemia with encrusted, healed lesions over both upper and lower limbs. Abdominal examination did not reveal any abnormalities. After submitting to routine complete blood count (CBC), malarial parasite (MP), blood cultures and line tip cultures, the patient was given empiric vancomycin injection. Ultrasound and CXR were negative at that time. Serum antineutrophil cytoplasmic antibody (ANCA) or antiproteinase 3 (PR3) were positive for cytoplasmic pattern on indirect immunoflourescense.
After staying afebrile for 3 days, the patient started to have spiking fever and became confused and drowsy. Repeat CXR showed worsening infiltrates and he was started on intravenous Piperacillin/Tazobactam plus Fluconazole, for positive blood cultures for Candida Albicans and steroid were being tapered. Echocardiogram was negative for vegetations.
Cerebrospinal fluid (CSF) examination, due to neck rigidity, revealed sugar of 27 mg/dl and proteins of 220 g/l and cell count of 40 with 95% neutrophils and 5% lymphocytes. An abdominal CT done due to the presence of air found on routine abdominal X-ray, revealed gas within the kidney and perinephric tissues.
The patients condition got progressively worse, requiring mechanical ventilation due to hypoxia. The presence of gas within and around the kidney entailed right nephrectomy (Fig.1B), histology of which revealed extensive infarction with gas filled spaces (Fig.1C) and numerous broad, aseptate, right angle branching fungal hyphae consistent with mucormycosis (Fig.1D). Focally, a few viable glomeruli showed organized crescents. The nephrectomy specimen was fixed in formalin and antibiotics were switched to Vancomycin, Imipenem and Amphotericin, but the patients condition continued to deteriorate post-operatively and he died three days after nephrectomy.
DISCUSSION
The term emphysematous pyelonephritis (EPN) is used to describe the presence of renal parenchymal gas formation1,2. Risk factors for this condition include diabetes mellitus (DM), urinary tract obstruction and urinary anomalies1-11.
Average patients age at the onset of EPN was 55 years, with a range of 19 to 81 years3. Women outnumbered men in nearly all reports, presumably owing to their increased susceptibility to urinary infection. It more commonly involves left kidney than the right and is bilateral only in 7%. Occasionally, it involves both kidneys sequentially rather than concurrently. Only three cases of EPN in a solitary kidney have been reported1. In contrast to the above findings, our patient was young, 18-years of age, of male gender and EPN involved the right kidney.
Three factors are postulated to be essential for spontaneous gas formation within the kidney: 1) obstruction of the urinary tract, 2) uncontrolled DM, and 3) gas producing organisms. Diabetes and obstruction have been documented in more than 80% and 40% of the reported cases, respectively1,6, while in non-diabetic patients, EPN is invariably associated with ureteric obstruction1. Escherichia coli accounts for the majority of cases, but other gram-negative uropathogens have been implicated as well1-10. Infrequently, gram-positive organisms have also been reported1. Occasionally, other organisms including Candida albicans have been found11. The mechanism of gas formation involves fermentation of glucose by gas producing organisms with production of carbon dioxide and hydrogen7. In our case, blood cultures were negative for bacteria but grew Candida albicans, and the nephrectomy specimen was fixed in formalin, hence tissue culture could not be done.
Regarding pathogenesis of this rare form of pyelonephritis, a number of theories have been proposed: glucose fermentation by bacteria in glucose rich environment in DM and the impaired host tissue response7.
It has been suggested that gas formation may not be associated with infection11.
The diagnosis depends on a constellation of clinical findings, laboratory results and the characteristic radiological findings of gas within the renal parenchyma, collecting system and perinephric space1,2.
The clinical presentation in most cases reviewed usually suggested severe acute pyelonephritis1.
Prompt radiologic examination is the gold standard to diagnose EPN. The most common radiologic patterns were gas collections in the renal parenchyma and perirenal tissues, as demonstrated by a plain abdominal radiograph and intravenous pyelography (IVP). Less common but characteristic patterns include mottled gas appearance and crescent formation.
Among the various radiologic procedures, the plain abdominal film revealed the presence of gas in 33% of cases1. In our patient, plain abdominal radiography was not performed. Instead, our patient underwent plain CT, which detected the gas. This imaging technique defines the extent of gas distribution more readily and accurately. The main pathologic features of EPN have been reported as severe acute and chronic necrotizing pyelonephritis with multiple cortical abscesses; other features reported include papillary necrosis, vascular thrombi and features of diabetic nephropathy; infarction has been reported in 3% of the cases1. Our case showed a completely infracted kidney with loss of corticomedullary distinction.
Management of EPN is controversial1,7-10. Different therapeutic options are available including medical, surgical or both. The mortality rate in medically managedpatients is greater than in those managed surgically or combined medical and surgical treatment7-10. Traditionally, nephrectomy has been the treatment of choice, however, the recent advent of interventional radiologic procedures has allowed successful renal preservation using a percutaneous drainage procedure. Treatment should be individualized according to the severity of the condition and the overall status of the patient1.
The prognosis of the condition has improved in recent years from most forms of treatment. The most striking reduction in mortality has been seen with surgical and combined modes of treatment. Early and prompt diagnosis of the condition and early institution of appropriate therapy are of critical importance in cases of EPN, as delay can jeopardize the patients kidney or even survival of the patient1.
References
1. Michaeli J, Mogle P, Perlberg S, Heiman S, Caine M. Emphysematous pyelonephritis. J Urol 1984;131(2):203-208 [ Links ]
2. Wan YL, Lee TY, Bullard MJ, Tsai CC. Acute gas producing bacterial renal infection: correlation between imaging findings and clinical outcome. Radiology 1996;198(2):433-438 [ Links ]
3. Shethy S. Emphysematous pyelonephritis (EPN).[Internet] 2012 [updated 2012, Jul; cited 2013, May 22].Available from: http://emedicine.medscape.com/article/2029011-overview
4. Shahatto N, al Awadhi NZ, Ghazali S. Emphysematous pyelonephritis: surgical implications. Br J Urol 1990; 66(6):572-574 [ Links ]
5. Shokeir AA, El-Azab M, Mohsen T, El-Diasty T. Emphysematous pyelonephritis: a 15-year experience with 20 cases. Urology 1997;49(3):343-346 [ Links ]
6. Pontin AR, Barnes RD, Joffe J, Kahn D. Emphysematous pyelonephritis in diabetic patients. Br J Urol 1995;75(1):71-74 [ Links ]
7. Huang JJ, Chen KW, Ruaan MK. Mixed acid fermentation of glucose as a mechanism of emphysematous urinary tract infection. J Urol 1991;146(1):148-151 [ Links ]
8. Corr J, Gleeson M, Wilson G, Grainger R. Percutaneous management of emphysematous pyelonephritis. Br J Urol 1993;71(4):487-488
9. Rathod KR, Narlawar RS, Garg A, Lolge S. Percutaneous conservative management of emphysematous pyelonephritis. J Postgrad Med 2001;47(1):66 [ Links ]
10. Chen MT, Huang CN, Chou YH, Huang CH, Chiang CP, Liu GC. Percutaneous drainage in the treatment of emphysematous pyelonephritis: 10-year experience. J Urol 1997;157(5):1569-1573 [ Links ]
11. Kamaliah MD, Bhajan MA, Dzarr GA. Emphysematous pyelonephritis caused by Candida infection. Southeast Asian J Trop Med Public Health 2005;36(3):725-727 [ Links ]
Professor Muhammed Mubarak
Histopathology Department,
Sindh Institute of Urology and Transplantation,
Karachi-74200, Pakistan,
E-mail: drmubaraksiut@yahoo.com
Email address:
Conflict of interest. None declared
Received for publication: 14/03/2013
Accepted: 15/05/2013


{kind=link}