










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.2 Lisboa abr. 2013
EDITORIAL
COSMOS: European evaluation and evolution of CKD-MBD
The Portuguese participation in the COSMOS project
Aníbal Ferreira1, José Luis Fernández-Martin2, Jorge B. Cannata-Andia2
1 Nephrology Department, Hospital Curry Cabral and Faculdade de Ciências Médicas, Universidade Nova de Lisboa, Lisboa, Portugal (National COSMOS coordinator for Portugal).
2 Bone and Mineral Research Unit, Instituto Reina Sofia de Investigation, REDinREN del ISCIII, Hospital Universitário Central de Asturias, Universidade de Oviedo, Oviedo, Asturias, Spain
In a time of political, social and economic crisis we face frequent movements against the European spirit of solidarity, partnership and international cooperation. In moments like this, the results of a study like COSMOS are particularly relevant, because they overpass the nephrology clinical results and illustrate the advantages of a broad scientific European cooperation.
COSMOS (current management of secondary hyperparathyroidism: a multicentre observational study) was designed to survey bone mineral disturbances in the haemodialysis population in Europe and the current clinical practice in Europe for the prevention, diagnosis and treatment of secondary hyperparathyroidism in haemodialysis patients1. This was a multicentre, open, prospective study collecting clinical information and outcome data from 5860 European haemodialysis patients. COSMOS was a non-interventional and observational study, without any subject contact (all data was collected from medical records).
Several aspects from the protocol design have contributed to the unique characteristics of the COSMOS study and to the relevance of its results, namely:
Large European population of prevalent (> 1 year) and incident (< 1 year) haemodialysis patients;
20 European countries were included, allowing the comparison of different zones (Mediterranean versus non-Mediterranean countries; East versus West European countries);
The number of sites and of patients was proportional to the haemodialysis population of each country;
293 European dialysis centres were randomly selected after stratification for public/private units and hospital based versus non-hospital based units;
Each centre recruited the same number of randomized patients (20);
The baseline patients lost to follow-up (between 15% and 30%) were replaced by new patients (< 1 year of haemodialysis) randomized from the same centre; Thus, there was always almost the same number of subjects followed over time and, due to the mortality and transplantation rates, the incident patients were almost 30%; In total, 4500 baseline patients and 2297 replacement patients were evaluated in COSMOS.
In addition, a survey of per centre clinical practices, including which targets for each parameter selected by the unit were considered, the frequency of the evaluation and, more important, the evolution/modification of these parameters over the 3 years duration of the study, was done. This approach allowed the long term evaluation of the utility and applicability of new targets and new guidelines, as is clearly illustrated by the substitution of the K/DOQI2,3 by the K/DIGO guidelines4, that was observed in the majority of the centres during the COSMOS duration;
This design of the study, which was strictly followed by the investigators, contributed to the important results of the COSMOS study illustrated by the 23 scientific presentations in congresses (including the Late breaking clinical trials session presented during the latest ERA-EDTA 50th Congress in Istanbul, and 2 communications to the recent World Congress of Nephrology, in Hong Kong, and the 5 manuscripts already published or accepted for publication.
The primary objectives from COSMOS were: 1) to estimate the prevalence of Kidney Disease Outcomes Quality Initiative (K/DOQI) guideline achievement in a representative sample of European haemodialysis patients; 2) to estimate the association of parathyroid hormone, calcium and serum phosphorous K/DOQI achievements, and overall and cardiovascular mortality; 3) to characterize the longitudinal changes in bone mineral markers (based in the 6 month repeated evaluation of all the clinical and laboratory data).
The secondary objectives of COSMOS had been: 1) to estimate the association between the achievement of the PTH, calcium and phosphorous K/DOQI serum levels and cardiovascular outcomes, parathyroidectomy, bone fractures, vascular calcifications, vascular access patency; 2) to evaluate the association of low albumin and anaemia, with mortality and clinically relevant events.
During the 3 years of the COSMOS study (2005-2007), the guidelines from K/DOKI were significantly modified by the new K/DIGO proposal, which seem to have diverse impact in the clinical practice of different European zones.
The first analysis of the baseline results from the COSMOS population was already published in a very interesting manuscript titled: COSMOS: the dialysis scenario of CKD-MBD in Europe 5, showing important variations in CKD-MBD diagnosis and therapy across Europe.
Some of the more interesting results from this baseline European population comparison are:
The confirmation that the European haemodialysis population is elderly (mean age approximately 65 years old) and have a long dialysis vintage (the later was more evident in Mediterranean versus non-Mediterranean countries and in West versus East European countries;
The high prevalence of diabetes (almost one third of the patients);
More than 2/3 of the patients presented already, at baseline, relevant cardiovascular morbidity;
Patients from the former Eastern countries were younger and had lower prevalence of diabetes;
Patients from the former Eastern countries showed a more deficient control of the CKD-MBD bone and mineral disturbances;
Almost one half of the patients received active vitamin D, but with significant differences between zones: In Mediterranean countries calcitriol use predominated, but in non-Mediterranean countries the majority of patients were under alfacalcidol therapy.
Also, the criteria used to decide about performing parathyroidectomy were different in the basal study population: In Mediterranean countries the level of parathyroid hormone considered to perform a parathyroidectomy was significantly higher than in non-Mediterranean countries.
In Portugal, the nephrology community has to be proud of its participation in such an interesting study.
The number of Portuguese facilities that participate was 110% of the planned value.
Concerning the number of patients, 101.5 of the planned patients were included in COSMOS.
Even more important, this number of patients was maintained during the 3 years of the protocol, reflecting a high compliance, from both the patients and the investigators, with this scientific project.
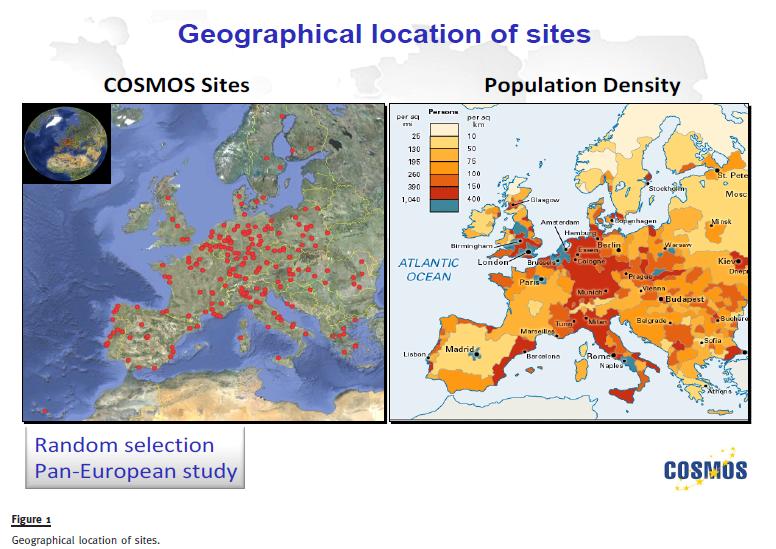
Figure 1
COSMOS is the largest protocol ever performed to evaluate the prevention, diagnosis and therapy of CKD-MBD.
In the next years many other manuscripts and scientific communications will arise from the COSMOS analysis.
We are honoured by the opportunity that has been given to the Portuguese Nephrology Community to be involved in such an interesting and promising study.
References
1. Cannata-Andia JB, Fernández-Martin JL, Zoccali C, et al. Current management of secondary hyperparathyroidism: a multicenter observational study (COSMOS). J Nephrol 2008;21(3):290-298 [ Links ]
2. National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003;42:S70-S77 [ Links ]
3. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int 2009;113(Suppl):S1-S130 [ Links ]
4. Moe S., DrüekeT, Cunningham J, et al. Definition, evaluation and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcome (KDIGO). Kidney Int 2006;69(11):1945-1953 5. [ Links ] Fernández-Martin J, Carrero JJ, Benedik M, et al. COSMOS: the dialysis scenario of CKD-MBD in Europe. Nephrol Dial Transplant 2012 Nov 19 [Epub ahead of print] [ Links ]
Prof Aníbal Ferreira
Nephrology Department, Hospital Curry Cabral
Rua da Beneficência, nº8, 1069-166
Lisboa, Portugal
E-mail: anibalferreira@netcabo.pt
Conflict of interest statement. None declared.
Received for publication: 11/06/2013
Accepted: 14/06/2013


{kind=link}