










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.1 Lisboa jan. 2013
Successful use of intravenous immunoglobulin in the treatment of resistant lupus nephritis
Imunoglobulina intravenosa eficaz no tratamento de nefrite lúpica resistente
Patrícia Cotovio, Cristina Silva, Nuno Afonso, Fátima Costa, Armando Carreira, Mário Campos
Nephrology Department, Centro Hospitalar e Universitário de Coimbra. Coimbra, Portugal
ABSTRACT
Background: Renal involvement in systemic lupus erythematosus is a major factor of morbidity/mortality and a significant prognostic determinant. Despite the high rates of remission with current immunosuppressive therapies, management of refractory lupus nephritis is still cumbersome. In these cases, intravenous immunoglobulin may be a suitable option, regardless of the scarcity of experience with long-term use.
Case report: We present the case of a 35-year-old female with a diagnosis of systemic lupus erythematosus since 1999, at the age of 23. In 2002, due to a nephrotic syndrome, a kidney biopsy was performed, which revealed WHO class IV lupus nephritis. She underwent immunosuppression with prednisolone and cyclophosphamide, with subsequent conversion to azathioprine. Proteinuria decreased to subnephrotic levels. In 2005, a nephrotic syndrome relapse occurred and kidney biopsy was repeated, with a similar result. After conversion from azathioprine to mycophenolate mofetil, proteinuria decreased to subnephrotic levels. At the end of 2006, a nephrotic syndrome relapse accompanied by arthralgia, azotaemia, leukopaenia and anaemia led to a third biopsy. The diagnosis was again the same, with no sclerotic lesions. Intravenous immunoglobulin was initiated in a protocol of monthly courses of 400mg/Kg/day during 5 consecutive days, maintaining prednisolone and mycophenolate mofetil. She achieved partial and complete remission after the third and tenth courses, respectively. The treatment scheme of immunoglobulin became quarterly from the second year until today. In 2010, she became pregnant and mycophenolic acid was replaced by azathioprine.In the last trimester of pregnancy proteinuria worsened, thus delivery was induced at the 32nd week. Nowadays the patient is in complete remission of nephritis, without extrarenal manifestations of lupus and no adverse effects of intravenous immunoglobulin.
Conclusion: Intravenous immunoglobulin has been effectively used in a broad spectrum of lupus manifestations. As this case illustrates, it may be an option in the treatment of lupus nephritis resistant to conventional immunosuppressive therapy. Its long-term use appears to be safe.
Key-Words: Immunosuppression, intravenous immunoglobulin, lupus nephritis.
RESUMO
Introdução: O envolvimento renal no lupus eritematoso sistémico é um fator determinante de morbimortalidade e um importante marcador de prognóstico. Apesar das elevadas taxas de remissão alcançadas com as terapias imunossupressoras atuais, a abordagem da nefrite lúpica refratária permanece um desafio. A imunoglobulina intravenosa pode ser uma alternativa nestes casos, embora a experiência com a sua administração prolongada seja limitada.
Caso clínico: Apresentamos o caso de uma doente de 35 anos de idade com lupus eritematoso sistémico diagnosticado em 1999, aos 23 anos. Em 2002, por síndrome nefrótica, realizou biópsia renal que revelou nefrite lúpica classe IV OMS. Iniciou imunossupressão com prednisolona e ciclofosfamida, com conversão posterior a azatioprina. A proteinúria diminuiu para níveis subnefróticos. Em 2005, por recidiva da síndrome nefrótica repetiu biópsia renal, que foi sobreponível à anterior. Fez conversão de azatioprina para micofenolato de mofetil e a proteinúria reduziu para valores subnefróticos. Em finais de 2006, nova recidiva de síndrome nefrótica associada a artralgia, azotemia, leucopenia e anemia condicionou uma terceira biópsia. O diagnóstico foi o mesmo, sem lesões de esclerose. Iniciou imunoglobulina intravenosa num protocolo de ciclos mensais de 400mg/Kg/dia durante 5 dias consecutivos, mantendo prednisolona e micofenolato de mofetil. Alcançou remissão parcial e completa após o terceiro e décimo ciclos, respetivamente. O esquema de imunoglobulina passou a trimestral após o primeiro ano. Em 2010 engravidou, tendo-se convertido o micofenolato de mofetil para azatioprina. No último trimestre da gravidez agravou a proteinúria e o parto foi induzido à 32ª semana. Atualmente a doente apresenta remissão completa da nefrite, ausência de manifestações extra-renais de lúpus ou de efeitos adversos da imunoglobulina intravenosa.
Conclusão: A imunoglobulina intravenosa tem eficácia documentada num amplo espectro de manifestações de lúpus. Pode ser uma opção nos casos de nefrite lúpica resistente aos imunossupressores convencionais. A sua administração prolongada parece ser segura.
Palavras-Chave: Imunossupressão, imunoglobulina intravenosa, nefrite lúpica.
INTRODUCTION
Systemic lupus erythematosus (SLE) is a prototypical human autoimmune disease of unknown aetiology, characterised by intense inflammation and multiple organ damage. Renal involvement occurs in up to 60% of patients with SLE, and lupus nephritis (LN) remains a predominant cause of morbidity and mortality in SLE. Globally, 25% of patients with LN develop end-stage renal disease (ESRD) at 10-year follow-up1,2.
Despite the strong benefit of the current immunosuppressive drugs such as corticosteroids, azathioprine (AZA), cyclophosphamide (CYC) or mycophenolate mofetil (MMF), their toxicity levels are not negligible. Further, approximately 20% of patients do not achieve a response under current induction protocols3. To surpass these concerns, and with the increasing knowledge of SLEs immunopathogenesis, novel immunotherapeutic strategies have been tried.
Intravenous immunoglobulin (IVIG) therapy modulates autoimmune diseases by interacting with various Fc γ receptors. In SLE, additional mechanisms include inhibition of complement-mediated damage, modulation of cytokines and cytokine antagonists production, modulation of T and B-lymphocyte function, induction of lymphocytes and monocytes apoptosis, downregulation of autoantibody production, manipulation of the idiotype network and neutralisation of pathogenic autoantibodies4-6. IVIG has been successfully used to treat severe complications of SLE. such as refractory thrombocytopaenia, pancytopaenia, central nervous system involvement, secondary antiphospholipid syndrome and LN4. There are many reports on the beneficial effect of IVIG treatment in resistant LN7-11, reducing immune deposits in the kidney, reducing proteinuria, improving kidney function, and reducing corticosteroid dosage11.
In this report we present a successful use of IVIG in treatment of resistant WHO class IV LN.
CASE REPORT
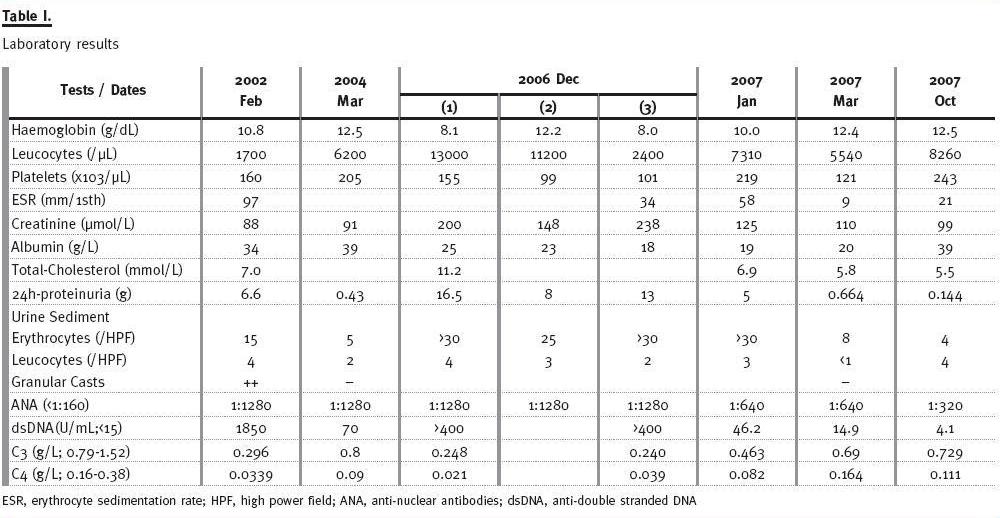
We present the case of 35-year-old, Caucasian, female, married and a lawyer by profession. She had a diagnosis of SLE established in 1999, at the age of 23, based on the American College of Rheumatology criteria: polyarthritis, malar rash, photosensitivity and immunologic disorders [anti-nuclear antibodies (ANA; titer 1:1280), anti-double stranded DNA (dsDNA; titer 1284U/mL) and hypocomplementaemia (C3, C4 and CH100)]. At that time, she had no renal or haematologic disorders. She started therapy with oral glucocorticoid, AZA, platelet antiaggregant, and maintained follow-up via Internal Medicine appointments. In April 2001, a flare (alopecia and malar rash exacerbation) required an increase of deflazacort (DFC) and AZA dosage. Chloroquine was initiated, as well as a 100-day course of thalidomide, with complete resolution of these symptoms. The patient became clinically stable until February 2002, when she developed malleolar and palpebral oedema and foamy urine. Her laboratory tests (Table I) were consistent with SLE flare associated with full nephrotic syndrome. She was started on a 3-day course of 1g intravenous (IV) methylprednisolone (MTP) and IV diuretic therapy, with partial regression of the oedema and haematologic improvement [Haemoglobin (Hb) 12.2g/dL, leukocytes 8200 cells/μL, erythrocyte sedimentation rate (ESR) 77mm/1sth].
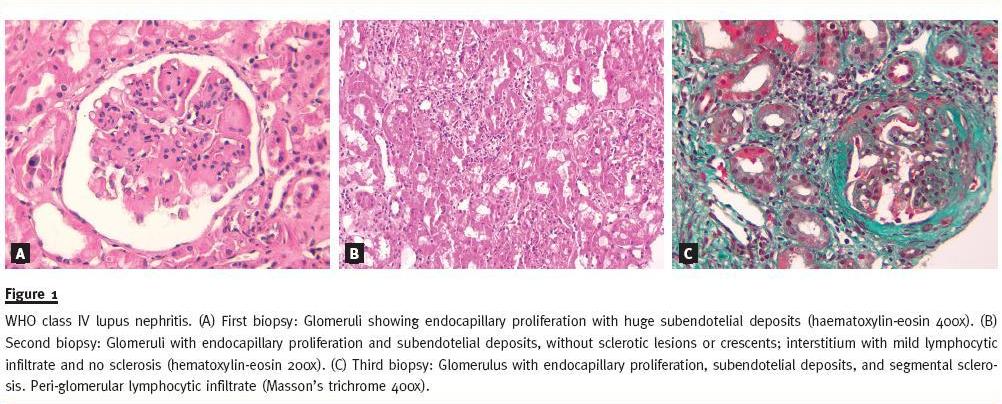
After transfer to our Nephrology department, a kidney biopsy was made that showed WHO class IV LN with a high degree of activity and mild degree of interstitial sclerosis (Fig. 1-A). She then underwent 6 monthly pulses of 1g IV CYC, followed by 6 quarterly pulses, along with oral prednisolone (PDN) 1mg/kg/day 8 weeks with subsequent tapering, and supportive therapy [angiotensin-converting-enzyme inhibitor (ACEI), aldosterone-receptor-antagonist (ARA), statin, platelet antiaggregant, calcium, vitamin D and gastric protector]. After the 4th CYC pulse, she achieved partial clinical remission, a condition sustained until the end of the 2nd year. In March 2004, she had no oedema; laboratory results (Table I) showed nearly complete clinical remission with only minor proteinuria and normal renal function.
However, there was only partial serologic remission: positive ANA, dsDNA and hypocomplementaemia. At that moment, she already had a cumulative CYC dosage of 214mg/kg (12g), so she continued immunosuppression with oral AZA 2mg/kg/day, DFC and supportive therapy.
She remained asymptomatic, with proteinuria 1-2g/24h until November 2004, when she had a nephrotic syndrome relapse (proteinuria 7.3g/24h) that did not respond to DFC rise. In February 2005, a kidney biopsy was performed showing similar results to the first one, without worsening of sclerosis (Fig.1-B). We switched AZA to MMF (aiming at 1g bid) and increased DFC to 42mg id. There was clinical improvement, with oedema regression and proteinuria reduction to 1-2g/24h; the active urinary sediment and immunologic disorders persisted.
In December 2006, she was admitted to the Nephrology ward with massive peripheral oedema. Laboratory tests (Table I), 2006-1) were again consistent with full LES flare with severe renal involvement. We maintained MMF 1g bid and performed 3 IV pulses of 1g MTP, followed by oral PDN 1mg/kg/day, along with supportive therapy. On discharge, after 2 weeks of therapy, the patient had no oedema and no haematologic disorders but maintained active urinary sediment along with azotaemia and serologic abnormalities (Table I), 2006-2).
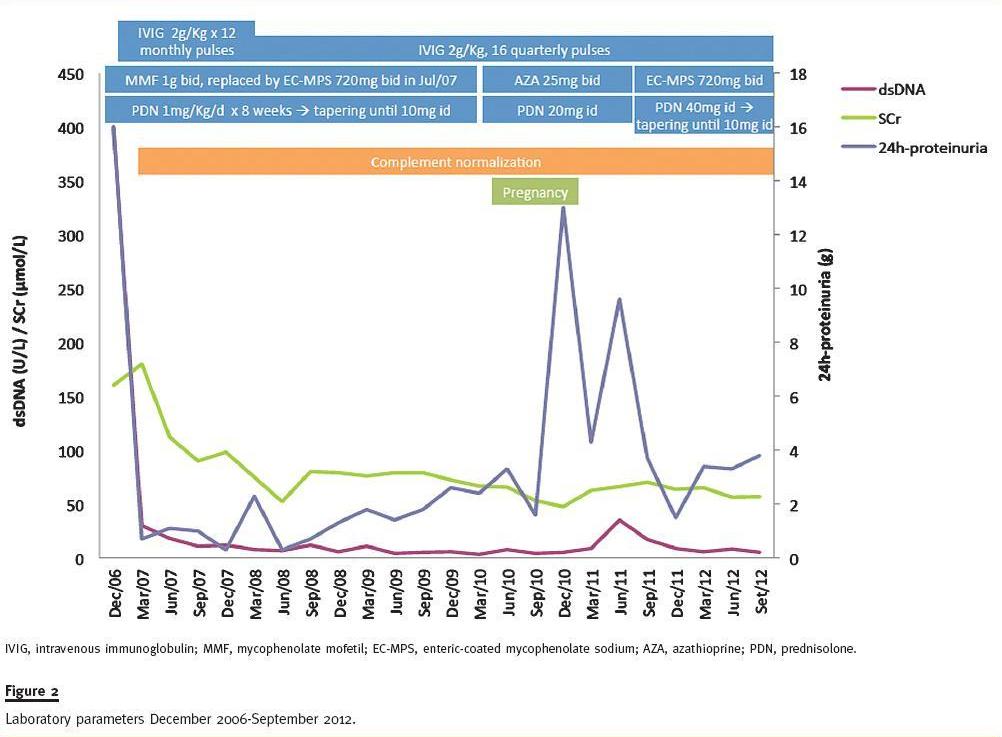
Four days later she was readmitted with disabling bilateral gonalgia and diarrhoea. Her complementary evaluation (Table I), 2006-3) revealed pancytopaenia, worsening of hypoalbuminaemia, azotaemia and proteinuria along with positive ANA, dsDNA and hypocomplementaemia. She continued with oral PDN 1mg/kg/day, temporarily interrupted MMF and initiated high dose IVIG (2g/kg) in a 5-day monthly protocol complemented by supportive therapy. After this course,we observed a dramatic clinical (resolution of the oedema and arthralgia) and laboratory improvement (Table I). The subsequent strategy was to provide 12 monthly courses of IVIG 2g/kg (120g) followed by quarterly courses throughout 3-4 years, plus PDN 1mg/kg/day during 8 weeks with subsequent tapering and MMF 1.5g id (a higher dosage worsened anaemia).
After the 2nd course, in February 2007, the patient seemed to have poor response to IVIG, so we performed a 3rd biopsy that was comparable to the previous (Fig.1-C). She achieved partial remission after the 3rd course, in March 2007 (Table I). Because of gastrointestinal intolerance, MMF was replaced by enteric-coated mycophenolate sodium (EC-MPS) 720mg bid. At the 10th course in October 2007, she was in complete remission (Table I). PDN attained 10mg id in November 2007. Figure 2 summarises the laboratory evolution.
In March 2010, she expressed desire to become pregnant, thus EC-MPS was converted to AZA 25mg bid, PDN was increased to 20mg id and ACEI and ARB were withdrawn. In May 2010, she became pregnant.
IVIG was given at weeks 10, 23 and 31, without adverse effects. Of note, since week 28 she presented peripheral oedema and the proteinuria increased to 3-4g/24h, with normotension. In January 2011, at week 32, proteinuria rose to 13g/24h, and delivery was induced with no complications for the mother or the newborn.
In July 2011, the patient maintained mild malleolar oedema and massive proteinuria (9.6g/24h), low level of C3 (0.604g/L) with normal C4, and positive ANA (1:320) and dsDNA(35). Thus, she was again converted to EC-MPS 720mg bid and augmented PDN to 40mg id, with a favourable response.
In the latest evaluation, in October 2012, she completed the 16th pulse of IVIG. She was clinically asymptomatic, normotensive, without peripheral oedema. Laboratory results showed normal blood panel, normal renal function (serum urea 4.6mmol/L and creatinine 56.8μmol/L), normal complementaemia (C3= 0.997 g/dL, C4= 0.187g/dL) and low titer of ANA (1:160) with negative dsDNA. Urine sediment was inactive with 24h-proteinuria of 3.8g.
Current therapy consists of EC-MPS 720mg bid, PDN 10mg id, furosemide 40mg bid, spironolactone 100mg id, irbesartan 300mg id, atorvastatin 20mg id, pantoprazole 20mg id, acetylsalicylic acid 100mg id, calcium 600mg + cholecalciferol 125U id, magnesium aspartate 1229.6mg id and alendronic acid 70mg bimonthly.
DISCUSSION
In the presented case, a female patient with SLE developed nephrotic syndrome, and the anatomopathological analysis of a kidney sample revealed a WHO class IV LN.
Treatment of LN usually involves two phases: 6 months of a more aggressive induction therapy which should be started as early as possible and aims to achieve renal remission, followed by a prolonged period of lower-dose maintenance therapy, aimed at ensuring durability of response, preventing renal flares and smoldering disease. Currently, there are a number of possible options for induction treatment of WHO or ISN/RPS class IV LN. KDIGO Clinical practice guideline for glomerulonephritis recommends, for initial therapy, corticosteroids combined either with CYC or MMF, and for maintenance therapy, AZA or MMF associated with low-dose oral corticosteroids12. However, back in 2006, and following landmark studies by the American National Institutes of Health (NIH), intermittent high dose IV CYC was generally adopted as the standard of care for class IV LN13,14.
The probability of response following induction therapy is similar whether using CYC or MMF, around 50% after the first year and 75%-80% after two years. Approximately 20% of patients do not reach a response under current induction protocols and between 5% and 25% can take as long as 24 months to achieve remission1,3. A better long-term prognosis is generally associated with attaining a clinical remission. Instead, a lack of response to induction therapy, as well as relapses of active nephritis predicts patient evolution towards ESRD15,16. Resistant patients should change treatment strategy1.
In our case, induction therapy with IV CYC plus oral PDN, based on the NIH studies protocols13,14, led to partial clinical, but not serological, remission.Improvements in proteinuria and renal function are the commonly adopted clinical criteria for remission, while serological parameters, such as normalization of reduced complement components or a decrease in dsDNA titer, may not be included due to the discrepant changes between serological and clinical parameters in some patients17.
Based on several reports18,19 that showed an overall patient survival benefit with AZA maintenance therapy, the patient continued immunosuppressive therapy _ with oral AZA. After about 2.5 years of partial remission, a nephrotic syndrome relapse occurred. In fact, recurrence of signs of renal activity after having partial or complete remission may occur more than 20 years after the first episode and tends to be associated with extrarenal symptoms and biochemical indicators of activity1.
Taking into account that changes in LN class have been described in as much as 50% of re-biopsies1, and to provide information on the degree of residual activity on the kidneys and the extent of chronic irreversible changes and its progression since the initiation of immunosuppressive treatment3, our patient was re-biopsied. At that time, cumulative dosage of CYC was superior to the maximal recommended (200mg/kg) to reduce the risk of gonadal toxicity. Therefore, supported by early studies that reported the efficacy of MMF in patients unresponsive to traditional immunosuppressive therapy20-22, AZA was switched to MMF. MMF has recently become a first-line drug for induction therapy in patients with class III and IV LN, concurrent with CYC1.
After 1.5 year of partial remission under MMF and PDN, our patient suffered a nephritic flare, a condition that is considered a stronger predictor of eventual development of irreversible deterioration of renal function16. Thus, the challenge was to select a new immunosuppressive drug efficient enough to remit LN but with minimal toxicity. However, there are no randomised studies to compare the efficacy/safety of different treatments in the case of recurrence1. In 2007, plausible therapeutic options were rituximab, calcineurin inhibitors or IVIG.
We decided to introduce high-dose IVIG, based on uncontrolled studies5,7-11that reported IVIG efficacy as salvage therapy of refractory LN.
In an Israeli cohort study, seven patients with biopsy proven class IV or V LN presenting nephrotic syndrome were treated with 1 to 6 courses of highdose IVIG after failing therapy with IV CYC and PDN7. They experienced decreases in proteinuria and improvement or resolution of the nephrotic syndrome. One patient had a complete remission, which persisted for at least three years. Only one patient had a relapse, which occurred 4 months after discontinuation of the IVIG.
In an Italian cohort, 12 patients with refractory NL were treated with 6-24 monthly courses of high-dose IVIG8. Progressive clinical improvement was observed in 11 patients, along with increased complement protein levels, decreases in auto-antibodies titers and marked improvements in renal function and proteinuria.
In another report, nine children with class IV or V LN unresponsive to CYC plus MTP were treated with high-dose IVIG9. Five of eight children with class IV nephritis saw marked improvement in renal function and decreases in IgG deposits on repeat biopsy, while the remaining three experienced a reduction in their class of nephritis. The sole patient with class V disease had a partial renal response.
In a Bulgarian cohort study10, 58 patients with refractory LN were treated with a low-dose IVIG regimen, 85 mg/kg/day on alternate days, for a total of three days, repeated quarterly for up to 7 years. At the conclusion of the study, 30% and 40% of the patients with LN achieved full and partial remission, respectively. Of non-responders, nearly all died or survived with ESRD, indicating the severity of disease in this cohort.
In twelve case reports, patients with class II, III, IV, or V LN received 1 or 2 courses of high-dose IVIG in combination with corticosteroids, with or without plasma exchange or cytotoxic agents. They recovered renal function with reductions in proteinuria and reduced immune deposits on repeat biopsy11.
The most commonly reported dosage of IVIG in LN is a high dose of total 2g/kg divided into five daily doses, in order to prevent the risk of adverse reactions4,6,11. There is no data on how long exogenous immunoglobulin remains present after administration and there is lack of consensus on dosing intervals. The optimal duration of therapy in LN is uncertain and depends on the patients response and objective signs of disease4,11. The largest clinical experience reported quarterly pulses for up to 7 years10.
Concerning toxicity, preparations rich in sucrose have been related to IVIG nephrotoxicity. The mechanism of renal injury may be osmotic nephrosis, with histological changes of vacuolisation of the proximal tubules with swelling and narrowing of the tubular lamina. Volume depletion, pre-existing renal disease and older age lower the threshold for renal toxicity5. Thromboembolic complications have also been reported in older patients with atherosclerotic risk factors3.
In our case, the result was excellent, with complete renal and serologic remission sustained for 4 years and with no adverse effects to report. The slight increase of proteinuria to subnephrotic levels may be attributed to underlying irreversible renal scarring17. We will probably continue quarterly IVIG courses as long as the patient maintains clinical remission without adverse effects.
During pregnancy a nephrotic flare occurred. Pregnancy in women with LN is associated with an increased risk of foetal loss and with worsening of the renal and extrarenal manifestations. The rate of successful pregnancies, excluding elective abortions, ranges from 65% to 92%. The rate of flares also varies widely ranging from 8% to 27% with some severe cases rarely evolving to maternal death23.
In conclusion, in this case of refractory WHO/ISN-RPS class IV LN the use of IVIG as a rescue therapy was effective and instrumental in achieving clinical remission and safe as maintenance therapy.
REFERENCES
1. Ruiz-Irastorza G, Espinosa G, Frutos MA, et al. Diagnosis and treatment of lupus nephritis. Consensus document from the systemic auto-immune disease group (GEAS) of the Spanish Society of Internal Medicine (SEMI) and the Spanish Society of Nephrology (SEN). Nefrologia 2012; 32(Suppl.1):1-35 [ Links ]
2. Lee YH, Woo JH, Choi SJ, Ji JD, Song GG. Induction and maintenance therapy for lupus nephritis: a systematic review and meta-analysis. Lupus 2010; 19(6):703-710 [ Links ]
3. Mok CC. Therapeutic options for resistant lupus nephritis. Semin Arthritis Rheum 2006;36(2):71-81 [ Links ]
4. Toubi E, Kessel A, Shoenfeld Y. High-dose intravenous immunoglobulins: an option in the treatment of systemic lupus erythematosus. Hum Immunol 2005; 66(4):395-402 [ Links ]
5. Orbach H, Tishler M, Shoenfeld Y. Intravenous immunoglobulin and the kidney – a two - edged sword. Semin Arthritis Rheum 2004; 34(3):593-601 [ Links ]
6. Gelfand EW. Intravenous immune globulin in autoimmune and inflammatory diseases. N Engj J Med 2012; 367(21):2015-2025 [ Links ]
7. Levy Y, Sherer Y, George J, et al. Intravenous immunoglobulin treatment of lupus nephritis. Semin Arthritis Rheum 2000; 29(5):321-327 [ Links ]
8. Francioni C, Galeazzi M, Fioravanti A, Gelli R, Megale F, Marcolongo R. Long- term IV Ig treatment in systemic lupus erythematosus. Clin Exp Rheumatol 1994; 12(2):163-168 [ Links ]
9. Lin CY, Hsu HC, Chiang H. Improvement of histological and immunological change in steroid and immunosuppressive drug-resistant lupus nephritis by high-dose intravenous gamma globulin. Nephron 1989; 53(4):303-310 [ Links ]
10. Monova D, Belovezhdov N, Altunkova I, Monov S. Intravenous Immunoglobulin G in the treatment of patients with chronic glomerulonephritis: clinical experience lasting 15 years. Nephron 2002; 90(3):262-266 [ Links ]
11. Wenderfer S, Thacker T. Intravenous immunoglobulin in the management of lupus nephritis. Autoimmune Dis 2012; 2012589359. doi: 10.1155/2012/589359 [ Links ]
12. NFK-KDIGO. Clinical practice guideline for glomerulonephritis. Kidney Int 2012;2(Suppl 2): 221-232 [ Links ]
13. Austin HA III, Klippel JH, Balow JE, et al. Therapy of lupus nephritis. Controlled trial of prednisone and cytotoxic drugs. N Engl J Med 1986;314(10): 614–619 [ Links ]
14. Illei GG, Austin HA, Crane M, et al. Combination therapy with pulse cyclophosphamide plus pulse methylprednisolone improves long-term renal outcome without adding toxicity in patients with lupus nephritis. Ann Intern Med 2001;135(4):248-257 [ Links ]
15. Houssiau FA, Vasconcelos C, DCruz D, et al. Early response to immunosuppressive therapy predicts good renal outcome in lupus nephritis. Arthritis Rheum 2004; 50(12):3934-3940 [ Links ]
16. Moroni G, Quaglini S, Maccario M, Banfi G, Ponticelli C. Nephritic flares are predictors of bad long-term renal outcome in lupus nephritis. Kidney Int 1996;50(6):2047-2053 [ Links ]
17. Chan TM. Lupus nephritis: induction therapy. Lupus 2005;14 Suppl 1:s27-32 [ Links ]
18. Contreras G, Pardo V, Leclercq B, et al. Sequential therapies for proliferative lupus nephritis. N Engl J Med 2004;350(10):971-980 [ Links ]
19. Mok CC, Ho CT, Chan KW, Law CS, Wong RW. Outcome and prognostic indicators of diffuse proliferative lupus glomerulonephritis treated with sequential oral cyclophosphamide and azathioprine. Arthritis Rheum 2002; 46(4):1003-1013 [ Links ]
20. Chan TM, Li FK, Tang CS, et al. Efficacy of mycophenolate mofetil in patients with diffuse proliferative lupus nephritis. Hong Kong-Guangzhou Nephrology Study Group. N Engl J Med 2000;343(16):1156-1162 [ Links ]
21. Chan TM, Tse KC, Tang CS, Mok MY, Li FK; Hong Kong Nephrology Study Group. Longterm study of mycophenolate mofetil as continuous induction and maintenance treatment for diffuse proliferative lupus nephritis. J Am Soc Nephrol 2005;16(4):1076-1084 [ Links ]
22. Ginzler EM, Dooley MA, Aranow C, et al. Mycophenolate mofetil or intravenous cyclophosphamide for lupus nephritis. N Engl J Med 2005;353(21):2219-2228 [ Links ]
23. Imbasciati E, Tincani A, Gregorini G, et al. Pregnancy in women with pre-existing lupus nephritis: predictors of fetal and maternal outcome. Nephrol Dial Transplant 2009;24(2):519-525 [ Links ]
Dr Patrícia Cotovio
Serviço de Nefrologia
Centro Hospitalar e Universitário de Coimbra
Quintas dos Vales
3041-801 São Martinho do Bispo
Coimbra, Portugal
E-mail: patriciacotovio@gmail.com
Acknowledgments: The authors would like to thank Dr Maria Fernanda Carvalho for providing the anatomopathological pictures.
Conflict of interest: None declared.
Received for publication: 01/12/2012
Accepted in revised form: 30/01/2013


{kind=link}
{kind=link}
{kind=link}