










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkAnálise Psicológica
Print version ISSN 0870-8231On-line version ISSN 1646-6020
Aná. Psicológica vol.35 no.4 Lisboa Dec. 2017
https://doi.org/10.14417/ap.1260
Professional quality of life in nurses: Contribution for the validation of the Portuguese version of the Professional Quality of Life Scale-5 (ProQOL-5)
Joana Duarte1
1CINEICC, Faculdade de Psicologia e de Ciências da Educação da Universidade de Coimbra
ABSTRACT
Job stress and burnout are highly prevalent in healthcare professionals, and nurses in particular. Given its deleterious consequences not only for professionals’ well-being but also for patients and organizations, it is important to have adequate measures to assess professional quality of life.
This study aimed to offer a contribution for the Portuguese validation of the Professional Quality of Life Scale-5. This scale was designed to measure three dimensions of professional quality of life: compassion satisfaction, burnout, and compassion fatigue.
The sample was composed by 390 nurses recruited from five public hospitals from Portugal north and center regions. Participants had on average 38.58 years of age (SD=9.10) and were mainly female, married, and practiced nursing in a variety of fields with an average of 15.66 (SD=9.09) years of practice. Results from the confirmatory factor analysis indicated that the original version of the scale had several problematic items and that a revised version showed superior model fit. In addition, results showed that female scored higher than men on Compassion Satisfaction. Also, nurses working in an oncology hospital had higher scores of Compassion Fatigue. Finally, higher scores of Burnout and Compassion Fatigue, and lower scores of Compassion Satisfaction, were associated with greater Depression, Anxiety, and Stress symptoms.
The ProQOL-5 is thus an adequate instrument to assess professional quality of life in nurses and may be valuable for designing effective interventions to tackle burnout and compassion fatigue, and promote satisfaction with one’s work.
Key words: Quality of life, ProQOL-5, Nursing, Confirmatory factor analysis, Validity, Portuguese.
RESUMO
O stress ocupacional e o burnout apresentam prevalências elevadas nos profissionais de saúde, e em enfermeiros em particular. Dadas as consequências negativas não apenas para o bem-estar dos profissionais mas também para os pacientes e para as organizações, é importante a existência de medidas adequadas para a avaliar a qualidade de vida profissional.
Este estudo tem como objetivo contribuir para a validação Portuguesa da Professional Quality of Life Scale-5. Esta escala foi desenvolvida para avaliar três dimensões da qualidade de vida profissional: Satisfação por Compaixão, Burnout, e Fadiga por Compaixão.
A amostra foi constituída por 390 enfermeiros recrutados em cinco hospitais públicos das regiões norte e centro de Portugal. Os participantes tinham, em média, 38.58 anos de idade (DP=9.10), eram maioritariamente do sexo feminino, casados, e exerciam enfermagem em diversas áreas, com uma média de 15.66 anos de experiência (DP=9.09).
Os resultados de uma análise fatorial confirmatória indicaram que a versão original da escala apresenta vários itens problemáticos e que uma versão revista da escala apresenta um ajustamento aos dados superior. Para além disso, os resultados demonstraram que os participantes do sexo feminino apresentaram pontuações superiores de Satisfação por Compaixão. Ainda, os enfermeiros que exercem a sua profissão em hospitais oncológicos apresentaram pontuações superiores de Fadiga por Compaixão. Por fim, pontuações mais elevadas de Burnout e Fadiga por Compaixão, e pontuações mais baixas de Satisfação por Compaixão, estão associadas a mais sintomas de Depressão, Ansiedade e Stress.
O ProQOL-5 é um instrumento adequado para avaliar a qualidade de vida profissional em enfermeiros e pode ser útil no desenvolvimento de intervenções eficazes para mitigar o burnout e a fadiga por compaixão, e para promover maior satisfação profissional.
Palavras-chave: Qualidade de vida, ProQOL-5, Enfermagem, Análise fatorial confirmatória, Validade, Português.
Introduction
Job stress and burnout are common in healthcare professionals (e.g., McCray, Cronholm, Bogner, Gallo, & Neill, 2008) and prevalence in nurses can be as high as 40% (Dominguez-Gomez & Rutledge, 2009; Sermeus et al., 2011; Vahey, Aiken, Sloane, Clarke, & Vargas, 2004). Although there are few studies in Portugal exploring burnout and work-related stress in nurses, a recent study with a large representative sample of Portuguese nurses concluded that the majority of nurses (49.4%) presented high levels of burnout (Marôco et al., 2016). These results are in accordance with a previous study with a large sample of Portuguese nurses (Jesus, Pinto, Fronteira, & Mendes, 2014).
Burnout has been described as a form of job stress characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment (Maslach, Schaufeli, & Leiter, 2001).
Several studies reported that stress and burnout in healthcare professionals are associated with several physical and mental health problems, such as such as fatigue, insomnia, hypertension, depression, anxiety, and low self-esteem (e.g., Maslach et al., 2001; Schulz et al., 2011). Burnout also decreases professional effectiveness and has been associated with suboptimal patient care (Shanafelt, Bradley, Wipf, & Back, 2002), and self-reported medical errors (West et al., 2006). In addition to objective errors in care, burnout may impact on the relationship with patients (Ratanawongsa et al., 2008). Burnout has been associated with decreased patient satisfaction, suboptimal self-reported patient care, and longer patient-reported recovery times (Shanafelt et al., 2002; Vahey et al., 2004).
In recent years, the term compassion fatigue has emerged in the literature to describe a related but different condition specific to professionals in helping contexts (healthcare professionals, teachers, police officers), who are in direct contact with the suffering of others (Figley, 1995). Compassion fatigue has been used interchangeably with secondary traumatic stress and vicarious trauma, because it is used to describe secondary stress reactions (e.g., re-experiencing the traumatic events, emotional numbness and avoidance of reminders, and persistent arousal) related to the provision of care to people who experienced some form of trauma or severe stress (Figley, 1995; Stamm, 2010). Given the nature of their work, nurses are particularly vulnerable to develop compassion fatigue (Joinson, 1992; Sorenson, Bolick, Wright, & Hamilton, 2016). Also less studied in the literature is the opposite end of job burnout and compassion fatigue, that is, the experience of fulfillment and satisfaction resulting from the work of caring for others, also known as compassion satisfaction (Stamm, 2010).
Having in mind these different dimensions of quality of life, Stamm (2005) developed the Professional Quality of Life Scale (ProQOL), which is now in its 5th version (Stamm, 2009). The ProQOL-5 was designed to assess professional quality of life, which is defined as the perceived quality regarding one’s work as a helper (Stamm, 2010). This self-report instrument is composed of three discrete subscales. The Burnout subscale measures feelings of hopelessness and difficulties in dealing with work or in doing one’s job effectively. The Compassion Fatigue/Secondary Traumatic Stress subscale refers to work-related trauma as a result of exposure to people who have experienced extremely or traumatically stressful events. Signs may include fear, sleep difficulties, intrusive images, or avoidance of reminders of the person’s traumatic experiences. Finally, the Compassion Satisfaction subscale measures the pleasure and satisfaction derived from doing a good work in helping others.
Despite being a relatively recent instrument, the ProQOL-5 is the most commonly used measure of the positive and negative effects of working with people who have experienced extremely stressful events, and has been used across different samples such as mental health caregivers (Sprang, Clark, & Whitt-Woosley, 2007), nurses (Hunsaker, Chen, Maughan, & Heaston, 2015), social workers (Bloomquist, Wood, Friedmeyer-Trainor, & Kim, 2016), volunteers working with trauma victims (Avieli, Ben-David, & Levy, 2015), and therapists working with traumatized patients (Sodeke-Gregson, Holttum, & Billings, 2013).
Recent studies have shown appropriate estimates of reliability of the ProQOL-5 in samples from different countries, such as Spain (Galiana, Arena, Oliver, Sansó, & Benito, 2017), Brazil (Galiana et al., 2017), Latvia (Circenis, Millere, & Deklava, 2013), China (Wu, Zhang, Yang, & Xu, 2014), Italy (Palestini, Prati, Pietrantoni, & Cicognani, 2009), Japan (Fukumori, Goto, Sato, & Sakamoto, 2016), and Israel (Samson, Iecovich, & Schvartzman, 2016).
Notwithstanding its wide use, there are few studies exploring the factorial structure of the scale. One published study using a sample of Italian accident and emergency workers provided a contribution for the factorial validity of the scale (Palestini et al., 2009). The results confirmed the validity of a revised version of the original tool, developed taking into account the results of confirmatory factor analyses and a detailed analysis of the content of the items. Also, a recent cross-cultural study with palliative care professionals from Spain and Brazil (Galiana et al., 2017) found evidence for overall psychometric appropriateness in both samples (e.g., adequate overall model fit and internal consistency).
Studies using the ProQOL questionnaire suggest that greater professional quality of life (more compassion satisfaction, and less burnout and compassion fatigue) is related to less depression and anxiety (e.g., Hegney et al., 2014; Yadollahi, Razmjooei, Jamali, Niakan, & Ghahramani, 2016), negative affect (e.g., Hegney, Rees, Eley, Osseiran-Moisson, & Francis, 2015; Zeidner, Hadar, Matthews, & Roberts, 2013), and perceived stress (e.g., Amin, Vankar, Nimbalkar, & Phatak, 2015), and greater general psychological and physical well-being (e.g., Mullira & Ssendikadiwa, 2016; Yadollahi et al., 2016), psychological resilience (Hegney et al., 2015), emotional intelligence, adaptive coping (Zeidner et al., 2013), mindfulness (e.g., Thomas & Otis, 2010), self-compassion (e.g., Duarte, Pinto-Gouveia, & Cruz, 2016), and empathy (e.g., Duarte et al., 2016; Gleichgerrcht & Decety, 2013, 2014).
The cultural adaption and validation study of the Portuguese version of the ProQOL-5 was conducted in a sample of 73 palliative caregivers (Carvalho, 2011). Despite being a preliminary contribution to the validation of the ProQOL to the Portuguese population, the sample used was small, specific to a palliative setting, and included several healthcare professions, such as physicians, nurses, and psychologists. Also, a detailed exploration of the factorial structure of the scale was not conducted.
This study
The aim of this study was to contribute to the validation of the Portuguese version of the ProQOL-5, using a sample of nurses. Specifically, we aimed to explore and confirm the factorial validity of the scale, given the scarcity of studies published thus far. We also aimed to explore possible differences in the ProQOL scores according to several sociodemographic and work-related variables.
Method
Participants and procedures
A total of 390 registered nurses from public hospitals participated in the study. This sample had a mean age of 38.58 years (SD=9.10), ranging between 22 and 60 years of age; the majority of participants were female (n=332; 87.60%) and married (n=202; 53.40%). Also, the mean years of schooling was 15.66 (SD=2.22). Participants practiced nursing in several fields, namely oncology (n=141; 36.20%), surgery (n=65; 16.70%), internal medicine (n=59; 15.50%), pediatrics (n=32; 8.20%), palliative care (n=20; 5.10%), emergency room (n=14; 3.60%), psychiatry (n=10; 2.60%), outpatient (n=8; 2.10%), family medicine (n=7; 1.80%), intensive care (n=4; 1.00%), continuity care (n=2; 0.50%), and other (n=19; 4.90%). Nurses had on average 15.62 (SD=9.09) years of practice.
Participants were recruited from five public hospitals from Portugal’s north and center regions, during 2014 and 2015. After approval of hospitals’ ethics committee, department chief nurses were directly contacted by the researcher who explained the study aims and the importance of participation. Department chief nurses were asked to present the study to the nurses in their services and to deliver the questionnaire pack to those who agreed to participate. The questionnaires were preceded by a page informing about the study aims, the importance of participation, and confidentiality. In line with the ethical requirements, it was emphasized that participants’ cooperation was voluntary and that their answers were confidential and would be used only for the purpose of this study. All participants provided their written informed consent. The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans was followed.
Measures
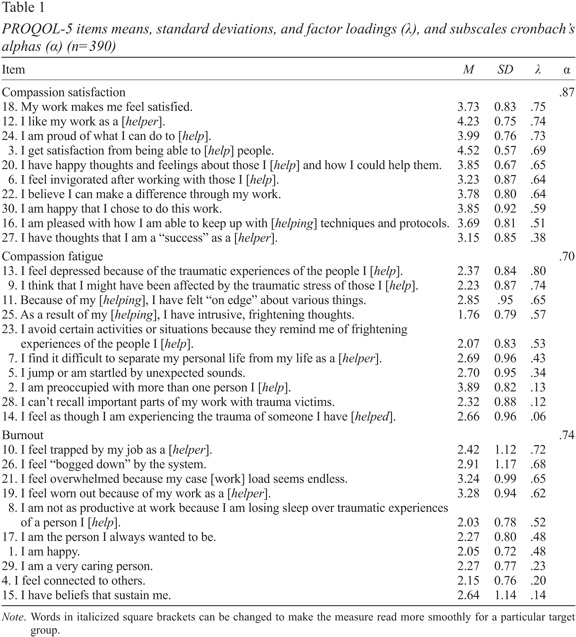
The Professional Quality of Life Scale, version 5 (ProQOL-5; Stamm, 2009; Portuguese version by Carvalho, 2011). The ProQOL-5 is a 30-item self-report measure composed by three subscales: Compassion Satisfaction, Burnout, and Secondary Traumatic Stress (STS). We will use the term ‘compassion fatigue’ to refer to this factor. Respondents are instructed to indicate how frequently each item was experienced in the previous 30 days, on a 5-point Likert scale (from 1=Never to 5=Very Often). Scoring requires summing the item responses for each 10-item subscale, and higher scores indicate higher levels of Compassion Satisfaction, Compassion Fatigue, and Burnout.
Depression, Anxiety, Stress Scale (DASS-21; Antony, Bieling, Cox, Enns, & Swinson, 1998; Lovibond & Lovibond, 1995; Portuguese version by Pais-Ribeiro, Honrado, & Leal, 2004). The DASS-21 comprises three subscales, each with seven items, measuring Depression, Anxiety, and Stress symptoms. Participants were asked to indicate the degree to which each statement applied to them in the last month. The DASS-21 uses a 4-point rating scale (0=Did not apply to me at all to 3=Applied to me very much, or most of the time). Validity and reliability of this scale across different samples has been well established (e.g., Lovibond & Lovibond, 1995; Pais-Ribeiro et al., 2004). Subscale scores were computed by calculating the sum of subscale item responses, and higher scores indicate higher levels of psychological symptoms.
Results
Confirmatory Factor Analysis
A Confirmatory Factor Analysis was conducted to test the factorial structure of the ProQOL-5. Specifically, we used structural equation modelling with the maximum likelihood estimation method. An evaluation of skewness (Sk) and kurtosis (Ku) was conducted to assess the assumption of normality of the items. There were no serious deviations from normality. To check for possible multidimensional outliers, the quadratic Mahalanobis distance (MD2) was used. Some outliers were identified; however, their removal did not change model fit, so these were included in the database.
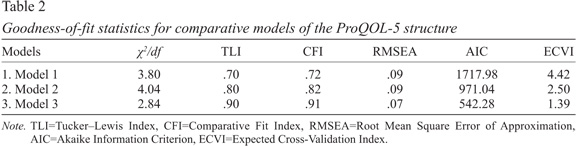
The models’ global adjustment was assessed through the following fit statistics: normed chi-square (χ2/degrees of freedom, df), Tucker–Lewis index (TLI), comparative fit index (CFI) and root mean square error of approximation (RMSEA). A very good fit is obtained when the χ2/df is 2 or lower, the CFI, and TLI are 0.90 or higher and the RMSEA is 0.10 or lower (Marôco, 2010). To compare the relative fit of the competing models, the Akaike information criterion (AIC) and the expected cross-validation index (ECVI) were used. The model with the smallest AIC and ECVI has the better fit (Marôco, 2010).
The first model tested (Model 1) was equivalent to the original factorial structure of the ProQOL-5 as proposed by the authors. As suggested in Table 1, this model presented a poor fit to the data. Taking into account the factor loadings of each item on the respective subscale (Table 1), as a next step we removed the items with standardized factor loadings<.50. This reduced model (Model 2) showed an increased fit to the data when compared to Model 1. Finally, we tested a third model in which item 8, originally from the Burnout scale, was relocated to the Compassion Fatigue scale, and item 11, originally from the Compassion Fatigue scale, was relocated to the Burnout scale. This decision was based on theoretical and statistical accounts. The content of item 8 (“I am not as productive at work because I am losing sleep over traumatic experiences of a person I [help]”) seems to describe a symptom associated with Compassion Fatigue. In support for this, Modification Indices (MI) also indicated a correlation between item 8 and the Compassion Fatigue latent variable. Regarding item 11, an examination of its content suggested that this item seems to more appropriately reflect Burnout as it expresses a sense of continuous ‘wear and tear,’ and not so much a consequence of secondary exposure to a traumatic event. Modification Indices also indicated a correlation between item 11 and the Burnout latent variable. Model fit for the final model is presented in Table 2, and indicates that this model presents the best fit to the data, when compared to Model 1 and Model 2. This model is composed by 19 items, with 9 items on the Compassion Satisfaction subscale, 5 items on the Compassion Fatigue subscale, and 5 items on the Burnout subscale.
Scale’s reliability and convergent validity
The composite reliability of the revised scale (Model 3) was very good (>.70), with .95 for Compassion Satisfaction, .88 for Compassion Fatigue and .91 for Burnout. Internal consistency assessed through Cronbach’s alpha was .88 for Compassion Satisfaction, .82 for Compassion Fatigue and .86 for Burnout. Convergent validity analysed through the average variance extracted (AVE) was also very good (>.05; Hair, Anderson, Tatham, & Black, 1998) for all the subscales: Compassion Satisfaction=.56; Compassion Fatigue=.59; Burnout=.66. Finally, we also conducted inter-correlations between the three scales. Results suggested that Compassion Satisfaction showed significant and negative correlations with Compassion Fatigue (r=-.22, p<.01) and Burnout (r=-.41, p<.01), and Compassion Fatigue was significantly and positively correlated with Burnout (r=.53, p<.01).
To explore the convergent validity of the measure we explored the correlations between the revised ProQOL-5 and Depression, Anxiety, and Stress symptoms assessed by the DASS-21. Depressive symptoms were significantly correlated with Compassion Satisfaction (r=-.30, p<.01), Burnout (r=.52, p<.01) and Compassion Fatigue (r=.34, p<.01); Anxiety symptoms were significantly associated with Compassion Satisfaction (r=-.16, p<.01), Burnout (r=.44, p<.01) and Compassion Fatigue (r=.49, p<.01); and Stress symptoms were also significantly associated with Compassion Satisfaction (r=-.14, p<.01), Burnout (r=.50, p<.01) and Compassion Fatigue (r=.43, p<.01). This pattern of correlations suggests that the revised ProQOL-5 has convergent validity.
In sum, results from the CFA suggest that the revised version of the ProQOL-5 is superior to the original 30-item version. However, given this is the first study to explore its factorial validity in a Portuguese sample, subsequent analyses were conducted with the original factor structure of the scale so results can be compared with previous studies.
Scores across demographic categories
There was a significant difference between male and female nurses on the Compassion Satisfaction score (t377=2.58, p=.013, d=.33), with women scoring significantly higher than men (M=38.37, SD=5.02 vs. M=35.70, SD=6.83). There were no significant differences between male and female nurses in Compassion Fatigue or Burnout. There were no significant differences between marital status and levels of Compassion Satisfaction (F4,377=0.38, p=.820), Burnout (F4,377=2.07, p=.084), and Compassion Fatigue (F4,377=1.62, p=.167).
No significant associations were found between age and Compassion Satisfaction (r=.09, p=.090), Burnout (r=-.04, p=.417), and Compassion Fatigue (r=-.02, p=.742). Also, no associations were found between years of practice and Compassion Satisfaction (r=.08, p=.127), Burnout (r=-.05, p=.346), and Compassion Fatigue (r=-.03, p=.582). However, we found a small but significant correlation between years in the current position and Burnout (r=.13, p=.012), but not Compassion Satisfaction (r=-.07, p=.212) nor Compassion Fatigue (r=.06, p=.256).
Scores across nursing specialty and work context
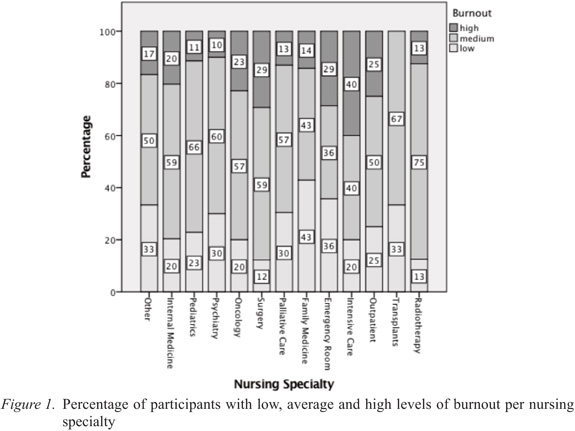
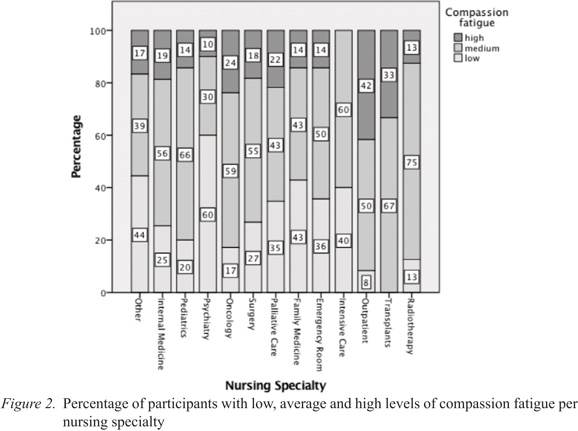
We were also interested in exploring the distribution of Compassion Satisfaction, Burnout, and Compassion Fatigue scores across nursing specialties. We conducted a one-way analysis of variance to explore whether levels of professional quality of life dimensions differed across nursing specialties. Results from this analysis suggested that there were no differences across specialties on levels of Compassion Satisfaction (F11,380=1.29, p=.229), Burnout (F11,380=1.14, p=.331), and Compassion Fatigue (F11,380=1.54, p=.116). However, post-hoc analysis using Fisher’s LSD test revealed several statistically significant differences (p<.05). For Compassion Satisfaction, we found that oncology nurse scored higher than surgery nurses (M=38.34, SD=5.64 vs. M=36.63, SD=4.74). For Burnout, palliative care nurses (M=23.05, SD=5.24) scored lower than internal medicine nurses (M=21.71, SD=5.52) and surgery nurses (M=26.49, SD=4.70). For Compassion Fatigue, we found that internal medicine nurses (M=25.64, SD=4.49) scored significantly higher than psychiatry nurses (M=22.40, SD=5.13). On the other hand, psychiatry nurses scored lower than paediatric nurses (M=26.00, SD=4.64), surgery nurses (M=25.92, SD=5.34), oncology medicine nurses (M=26.04, SD=3.88), and outpatient nurses (M=28.13, SD=3.72). We also found that outpatient nurses (M=28.13, SD=3.72) scored higher than family medicine nurses (M=22.57, SD=4.96) and family medicine nurses.
Figures 1 and 2 show the percentage of nurses with low, medium, and high scores of burnout and compassion fatigue for each nursing specialty. Participants were classified into low, medium, and high for each sub-subscale of the ProQOL-5 based on the cut scores for the 25th, 50th, and 75th percentile (Stamm, 2010). It should be taken into account that some specialties are underrepresented and thus these results should be interpreted with caution.
Finally, we also explored differences in professional quality of life between the two major categories of work places represented in our sample, namely general hospitals (n=207) and oncology hospitals (n=177). Results suggest a significant difference only in Compassion Fatigue (t382=-2.19, p=.029, d=.22), with nurses from oncology hospitals (M=26.13, SD=4.13) scoring significantly higher when compared to nurses from general hospitals (M=25.12, SD=4.95).
Discussion
This study represents the first attempt to explore the factorial structure and psychometric properties of the ProQOL-5 in a sample of Portuguese nurses. In addition, we also explored the relationship between professional quality of life and several demographic variables, such as age and gender, and work-related variables, such as years of practice, nursing specialty, and hospital affiliation.
Confirmatory Factor Analysis suggested that the three-factor structure of the ProQOL-5 originally proposed presented a poor fit to our data, with some problematic items. Specifically, positively worded items originally from the Burnout scale presented low factor loadings, and were thus excluded from the scale. It has been suggested that the use of positively – and negatively – worded items may introduce systematic measurement errors that disrupt analyses and interpretations of the results (e.g., Horan, DiStefano, & Motl, 2003). Also, an analysis of the content of such items suggests they may not be specific of burnout but have a more general meaning and thus may not aggregate with the other items of the Burnout scale. One item from the Compassion Satisfaction scale was also eliminated based on low factor loadings. Regarding the Compassion Fatigue scale, five items were also excluded based on low factor loadings. An analysis of the content of some of the items suggests that they may not be specific to Compassion Fatigue. For example, item 2 refers to the preoccupation regarding the recipients of help. However, it may be that preoccupation is not in the negative sense, but instead represents a positive aspect of concern and interest for the patients. In contrast, the items that presented higher factor loadings are more clearly related to Compassion Fatigue associated symptoms (e.g., being affected by traumatic experiences related to helping, hyperarousal, intrusive thoughts and feelings related to the traumatic experience, avoidance of reminders of the traumatic experience…).
In addition, two items that originally belonged to one scale were moved based on theoretical and statistical considerations. Specifically, item 8, which originally belonged to the Burnout scale was moved to the Compassion Fatigue scale. An analysis of the content of this item suggested that it may reflect a symptom of compassion fatigue rather than burnout. Item 11, which originally belonged to the Burnout scale was moved to the Compassion Fatigue scale. Again, a close examination of its content suggested that this item seems to more appropriately reflect burnout as it expresses a sense of continuous ‘wear and tear,’ and not so much a consequence of secondary exposure to a traumatic event.
Results from this analysis suggested that not all items included in the original version of the scale show acceptable psychometric properties and clear theoretical content and thus the exclusion of such items is advised. The model of the revised version of the scale, with 19 items and two relocated items, showed the best fit to the data. In addition, the internal consistency of the revised scale was superior to the Portuguese long version of the scale (Compassion Satisfaction: α=.60; Compassion Fatigue: α=.68; and Burnout: α=.63; Carvalho, 2011) and to the original version of the scale (Compassion Satisfaction: α=.88; Compassion Fatigue: α=.81; and Burnout: α=.75; Stamm, 2010).
The separation between the Burnout and Compassion Fatigue factors was also sustained by our results. Correlation analysis suggested that the two constructs only shared 28% of the variance. This result is slightly lower that the one found in the previous study of the Portuguese version of the ProQOL-5 (30%; Carvalho, 2011), and lower than the one found in a previous meta-analysis (48%; Cieslak et al., 2014).
In the present sample, there were significant differences between female and male nurses in Compassion Satisfaction scores, but not in Burnout or Compassion Fatigue. Research has produced mixed results regarding the role of gender on professional quality of life. In a recent meta-analysis, women exhibit more burnout than men (Purvanova & Muros, 2010), which was not found in the present study. Results for nurses in particular also seem to suggest more burnout (specifically emotional exhaustion) in women (Innstrand, Langballe, Falkum, & Aasland, 2011). Regarding studies that used the ProQOL-5, results from a large data bank found no significant differences across gender (Stamm, 2010), and a recent study found that men scored higher in Compassion Satisfaction, although with small effect sizes (Gleichgerrcht & Decety, 2013). We also failed to find an association between age and professional quality of life, a result consistent with some studies using the ProQOL (e.g., Stamm, 2010) but not others (e.g., Palestini et al., 2009).
The result that professional experience was not associated with professional quality of life is consistent with previous findings (Gleichgerrcht & Decety, 2013; Potter et al., 2010; Stamm, 2010). However, we found that more time in the current position was associated with greater levels of Burnout, which was not found in a previous study (Vargas, Cañadas, Aguayo, Fernández, & De la Fuente, 2014). Regarding other work-related variables, results suggested that nurses working in an oncology hospital presented higher scores of Compassion Fatigue, but no differences in Burnout or Compassion Satisfaction were found. Oncology nursing is one of the areas most affected by occupational stress (e.g., Barnard, Street, & Love, 2006; Potter et al., 2010). In addition to the well-documented stressors found in other areas (e.g., high workload, shift working), oncology nurses face additional challenges associated with the management of complex pathologies with poor prognosis, close and constant contact with patients who are in severe pain and approaching death, and difficult patient and family situations, which may put oncology nurses at greater risk of compassion fatigue (Najjar, Davis, Beck-Coon, & Doebbeling, 2009).
Finally, nurses that presented higher scores of Burnout and Compassion Fatigue, and lower scores of Compassion Satisfaction, also presented higher levels of Depression, Anxiety, and Stress symptoms. These results provide some support for the convergent validity of the measure, given that Burnout was particularly associated with Depression symptoms and Compassion Fatigue was particularly associated with Anxiety, as would be expected. In fact, there is a considerable overlap between burnout and depression and their distinction remains conceptually fragile (e.g., Bianchi, Schonfeld, & Laurent, 2015). Also, although trauma and stress-related disorders are now separated from anxiety disorders in the DSM-V, until the DSM-IV-TR they were included under the same category (American Psychiatric Association, 2000, 2013), reflecting a common underlying symptom structure.
Although this study reports promising findings, several limitations should be taken into account. Participants were mainly women, which limits the generalizability of the findings. However, the proportion of female and male nurses in our sample matches other international and national samples (e.g., Budden, Zhong, Moulton, & Cimiotti, 2013; Marôco et al., 2016). In addition, we used a convenience sample of hospitals and nurses which, by being a nonprobability sampling method, may not adequately represent the population. Also, it was not possible to conduct several measurements in different time points in order to assess test-retest reliability. Finally, this study did not include other instruments to explore convergent and divergent validity.
In conclusion, results from this study provide preliminary support for the use of a revised version of the ProQOL-5 as a reliable measure to assess professional quality of life in nurses. This scale is particularly suited to use in nursing, and in healthcare in general, given the specificity of its items, that were developed taken into account the consequences that may result from working as care providers to others in need. Also, the fact that this scale comprises not only the negative but also the positive aspects associated with work gives a broader and more complete perspective of professional quality of life. This may be particularly important for research purposes and also for designing interventions to increase healthcare professionals’ quality of life, that could aim not only to reduce burnout and compassion fatigue, but also promote a sense of satisfaction from the work of caring for others.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Arlington, VA: American Psychiatric Publishing. [ Links ]
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. [ Links ]
Amin, A. A., Vankar, J. R., Nimbalkar, S. M., & Phatak, A. G. (2015). Perceived stress and professional quality of life in neonatal intensive care unit nurses in Gujarat, India. Indian Journal of Pediatrics, 82, 1001-10015. doi: 10.1007/s12098-015-1794-3 [ Links ]
Antony, M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and community a sample. Psychological Assessment, 10, 176-181. [ Links ]
Avieli, H., Ben-David, S., & Levy, I. (2015). Predicting professional quality of life among professional and volunteer caregivers. Psychological Trauma: Theory, Research, Practice, and Policy, 8, 80-87. doi: 10.1037/tra0000066 [ Links ]
Barnard, D., Street, A., & Love, A. W. (2006). Relationships between stressors, work supports, and burnout among cancer nurses. Cancer Nursing, 29, 338-345. doi: 10.1097/00002820-200607000-00013 [ Links ]
Bianchi, R., Schonfeld, I. S., & Laurent, E. (2015). Burnout-depression overlap: A review. Clinical Psychology Review, 36, 28-41. doi: 10.1016/j.cpr.2015.01.004 [ Links ]
Bloomquist, K. R., Wood, L., Friedmeyer-Trainor, K., & Kim, H.-W. (2016). Self-care and professional quality of life: Predictive factors among MSW practitioners. Advances in Social Work, 16, 292-311. doi: 10.18060/18760 [ Links ]
Budden, J. S., Zhong, E. H., Moulton, P., & Cimiotti, J. (2013). Highlights of the national workforce survey of registered nurses. Journal of Nursing Regulation, 4, 10. doi: 10.1016/S2155-8256(15)30151-4 [ Links ]
Carvalho, P. (2011). Estudo da fadiga por compaixão nos cuidados paliativos em Portugal: Tradução e adaptação cultural da Escala Professional Quality of Life-5. Unpublished Master thesis. Universidade Católica Portuguesa, Porto. [ Links ]
Cieslak, R., Shoji, K., Douglas, A., Melville, E., Luszczynska, A., & Benight, C. C. (2014). A meta-analysis of the relationship between job burnout and secondary traumatic stress among workers with indirect exposure to trauma. Psychological Services, 11, 75-86. doi: 10.1037/a0033798 [ Links ]
Circenis, K., Millere, I., & Deklava, L. (2013). Measuring the professional quality of life among latvian nurses. Procedia-Social and Behavioral Sciences, 84, 1625-1629. doi: 10.1016/j.sbspro.2013.07.003 [ Links ]
Dominguez-Gomez, E., & Rutledge, D. N. (2009). Prevalence of secondary traumatic stress among emergency nurses. Journal of Emergency Nursing, 35, 199-204. doi: 10.1016/j.jen.2008.05.003 [ Links ]
Duarte, J., Pinto-Gouveia, J., & Cruz, B. (2016). Relationships between nurses’ empathy, self-compassion and dimensions of professional quality of life: A cross-sectional study. International Journal of Nursing Studies, 60, 1-11. doi: 10.1016/j.ijnurstu.2016.02.015
Figley, C. R. (1995). Compassion fatigue as secondary traumatic stress disorder: An overview. In C. R. Figley (Ed.), Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatised (pp. 1-20). New York, NY: Routledge. [ Links ]
Fukumori, T., Goto, T., Sato, H., & Sakamoto, H. (2016, July). Development, reliability, and validation of a Japanese nurse version of the Professional Quality of Life Scale (ProQOL-JN). [ Links ] Poster session presented at the meeting of the 31st International Congress of Psychology, Yokohama, Japan.
Galiana, L., Arena, F., Oliver, A., Sansó, N., & Benito, E. (2017). Compassion satisfaction, compassion fatigue, and burnout in Spain and Brazil: ProQOL validation and cross-cultural diagnosis. Journal of Pain and Symptom Management, 53, 598-604. Retrieved from http://dx.doi.org/10.1016/j.jpainsymman.2016.09.014 [ Links ]
Gleichgerrcht, E., & Decety, J. (2013). Empathy in clinical practice: How individual dispositions, gender, and experience moderate empathic concern, burnout, and emotional distress in physicians. PLoS ONE, 8, e61526. doi: 10.1371/journal.pone.0061526 [ Links ]
Gleichgerrcht, E., & Decety, J. (2014). The relationship between different facets of empathy, pain perception and compassion fatigue among physicians. Frontiers in Behavioral Neuroscience, 8, 243. doi: 10.3389/fnbeh.2014.00243 [ Links ]
Hair, J. E., Anderson, R. E., Tatham, R. L., & Black, W. C. (1998). Multivariate data analysis (5th ed.). Upper Saddle River, NJ: Prentice-Hall. [ Links ]
Hegney, D. G., Craigie, M., Hemsworth, D., Osseiran-Moisson, R., Aoun, S., Francis, K., & Drury, V. (2014). Compassion satisfaction, compassion fatigue, anxiety, depression and stress in registered nurses in Australia: Study 1 results. Journal of Nursing Management, 22, 506-518. doi: 10.1111/jonm.12160 [ Links ]
Hegney, D. G., Rees, C. S., Eley, R., Osseiran-Moisson, R., & Francis, K. (2015). The contribution of individual psychological resilience in determining the professional quality of life of Australian nurses. Frontiers in Psychology, 6, 1-8. Retrieved from http://dx.doi.org/10.3389/fpsyg.2015.01613 [ Links ]
Horan, P. M., DiStefano, C., & Motl, R. W. (2003). Wording effects in self-esteem scales: Methodological artifact or response style ?. Structural equation modeling: A Multidisciplinary Journal, 10, 435-455. doi: 10.1207/S15328007SEM1003_6
Hunsaker, S., Chen, H.-C., Maughan, D., & Heaston, S. (2015). Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. Journal of Nursing Scholarship, 47, 186-194. doi: 10.1111/jnu.12122 [ Links ]
Innstrand, S. T., Langballe, E. M., Falkum, E., & Aasland, O. G. (2011). Exploring within- and between-gender differences in burnout: 8 different occupational groups. International Archives of Occupational and Environmental Health, 84, 813-824. doi: 10.1007/s00420-011-0667-y [ Links ]
Jesus, E. H., Pinto, A. M., Fronteira, I., & Mendes, A. (2014). Estudo RN4CAST em Portugal: Percepção dos enfermeiros sobre burnout. Revista Investigação em Enfermagem, 2, 47-59. [ Links ]
Joinson, C. (1992). Coping with compassion fatigue. Nursing, 22, 116-121. [ Links ]
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343. doi: 10.1016/0005-7967(94)00075-U [ Links ]
Marôco, J. (2010). Análise de equações estruturais: Fundamentos teóricos, software & aplicações. Pêro Pinheiro: ReportNumber, Lda. [ Links ]
Marôco, J., Marôco, A., Leite, E., Bastos, C., Vazão, M. J., & Campos, J. (2016). Burnout em profissionais da saúde portugueses: Uma análise a nível nacional. Acta Médica Portuguesa, 29, 24-30. [ Links ]
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397-422. doi: 10.1146/annurev.psych.52.1.397 [ Links ]
McCray, L. W., Cronholm, P. F., Bogner, H. R., Gallo, J. J., & Neill, R. A. (2008). Resident physician burnout: Is there hope?. Family Medicine, 40, 626-632. [ Links ]
Mullira, R. S., & Ssendikadiwa, V. B. (2016). Professional quality of life and associated factors among Ugandan midwives working in Mubende and Mityana rural districts. Maternal and Child Health Journal, 20, 567-576. doi: 10.1007/s10995-015-1855-2 [ Links ]
Najjar, N., Davis, L. W., Beck-Coon, K., & Doebbeling, C. C. (2009). Compassion fatigue: A review of the research to date and relevance to cancer-care providers. Journal of Health Psychology, 14, 167-277. [ Links ]
Pais-Ribeiro, J. L., Honrado, A., & Leal, I. (2004). Contribuição para o estudo da adaptação portuguesa das Escalas de Ansiedade, Depressão e Stress (EADS) de 21 itens de Lovibond e Lovibond. Psicologia, Saúde e Doenças, 5, 229-239. [ Links ]
Palestini, L., Prati, G., Pietrantoni, L., & Cicognani, E. (2009). La qualità della vita professionale nel lavoro di soccorso: Un contributo alia validazione italiana della Professional Quality of Life Scale (ProQOL). Psicoterapia Cognitiva e Comportamentale, 15, 205-227. [ Links ]
Potter, P., Deshields, T., Divanbeigi, J., Berger, J., Cipriano, D., Norris, L., & Olsen, S. (2010). Compassion fatigue and burnout: Prevalence among oncology nurses. Clinical Journal of Oncology Nursing, 14, e56-62. doi: 10.1188/10.CJON.E56-E62 [ Links ]
Purvanova, R. K., & Muros, J. P. (2010). Gender differences in burnout: A meta-analysis. Journal of Vocational Behavior, 77, 168-185. doi: 10.1016/j.jvb.2010.04.006 [ Links ]
Ratanawongsa, N., Roter, D., Beach, M. C., Laird, S. L., Larson, S. M., Carson, K. A., & Cooper, L. A. (2008). Physician burnout and patient-physician communication during primary care encounters. Journal of General Internal Medicine, 23, 1581-1588. doi: 10.1007/s11606-008-0702-1 [ Links ]
Samson, T., Iecovich, E., & Schvartzman, P. (2016). Psychometric characteristics of the Hebrew version of the Professional Quality-of-Life Scale. Journal of Pain and Sympto Management, 52, 575-581. doi: 10.1016/j.jpainsymman.2016.03.019 [ Links ]
Schulz, M., Damkroger, A., Voltmer, E., Lowe, B., Driessen, M., Ward, M., & Wingenfeld, K. (2011). Work-related behaviour and experience pattern in nurses: Impact on physical and mental health. Journal of Psychiatric and Mental Health Nursing, 18, 411-417. doi: 10.1111/j.1365-2850.2011.01691.x [ Links ]
Sermeus, W., Linda, H. A., Koen, V. H., Anne, M. R., Peter, G., & Moreno-Casbas, M. T. (2011). RN4CAST consortium. BMC Nursing, 10. doi: 10.1186/1472-6955-10-6 [ Links ]
Shanafelt, T. D., Bradley, K. A., Wipf, J. E., & Back, A. L. (2002). Burnout and self-reported patient care in an internal medicine residency program. Annals of Internal Medicine, 136, 358-367. doi: 10.7326/0003-4819-136-5-200203050-00008 [ Links ]
Sodeke-Gregson, E. A., Holttum, S., & Billings, J. (2013). Compassion satisfaction, burnout, and secondary traumatic stress in UK therapists who work with adult trauma clients. European Journal of Psychotraumatology, 4, 1-10. doi: 10.3402/ejpt.v4i0.21869 [ Links ]
Sorenson, C., Bolick, B., Wright, K., & Hamilton, R. (2016). Understanding compassion fatigue in healthcare providers: A review of current literature. Journal of Nursing Scholarship, 48, 456-465. doi: 10.1111/jnu.12229 [ Links ]
Sprang, G., Clark, J. J., & Whitt-Woosley, A. (2007). Compassion fatigue, compassion satisfaction, and burnout: Factors impacting a professional’s quality of life. Journal of Loss and Trauma, 12, 259-280.
Stamm, B. H. (2005). The professional Quality of Life scale: Compassion satisfaction, Burnout, and compassion fatigue/secondary trauma scales. Latherville, MD: Sidran Press. [ Links ]
Stamm, B. H. (2009). Professional Quality of Life: Compassion satisfaction and fatigue – Version 5 (ProQOL). Retrived from http://www.proqol.org/uploads/ProQOL_5_English.pdf
Stamm, B. H. (2010). The Concise ProQOL Manual (2nd ed.). Pocatello, ID: ProQOL.org. [ Links ]
Thomas, J. T., & Otis, M . D. (2010). Intrapsychic correlates of Professional Quality of Life: Mindfulness, empathy, and emotional separation. Journal of the Society for Social Work and Research, 1, 83-98. doi: 10.5243/jsswr.2010.7 [ Links ]
Vahey, D. C., Aiken, L. H., Sloane, D. M., Clarke, S. P., & Vargas, D. (2004). Nurse burnout and patient satisfaction. Medical Care, 42, II57-I66. doi: 10.1097/01.mlr.0000109126.50398.5a [ Links ]
Vargas, C., Cañadas, G. A., Aguayo, R., Fernández, R., & De la Fuente, E. I. (2014). Which occupational risk factors are associated with burnout in nursing? A meta-analytic study. International Journal of Clinical and Health Psychology, 14, 28-38. doi: 10.1016/S1697-2600(14)70034-1 [ Links ]
West, C. P., Huschka, M. M., Novotny, P. J., Sloan, J. A., Kolars, J. C., Habermann, T. M., & Shanafelt, T. D. (2006). Association of perceived medical errors a prospective longitudinal study. Journal of the American Medical Association, 296, 1071-1078. Retrieved from http://dx.doi.org/10.5688/ajpe76224 [ Links ]
Wu, J.-M., Zhang, Y.-Q., Yang, Y., & Xu, Y. (2014). Evaluation of reliability and validity of Chinese version of Professional Quality of Life Scale for nurses. Journal of Shanghai Jiaotong University, 34, 1281-1285. doi: 10.3969/j.issn.1674-8115.2014.09.005 [ Links ]
Yadollahi, M., Razmjooei, A., Jamali, K., Niakan, M. A., & Ghahramani, Z. (2016). The relationship between Professional Quality of Life (ProQol) and general health in Rajaee Trauma Hospital Staff of Shiraz, Iran. Shiraz E-Medical Journal, 17, e39253. doi: 10.17795/semj39253 [ Links ]
Zeidner, M., Hadar, D., Matthews, G., & Roberts, R. D. (2013). Personal factors related to compassion fatigue in health professionals. Anxiety, Stress, and Coping, 26, 595-609. doi: 10.1080/10615806.2013.777045 [ Links ]
Correspondence concerning this article should be addressed to: Joana Duarte, CINEICC, Faculdade de Psicologia e de Ciências da Educação da Universidade de Coimbra, Rua do Colégio Novo, 3001-802, Coimbra, Portugal. E-mail: joana.fm.duarte@gmail.com
This study was supported by FCT – Fundação para a Ciência e Tecnologia, Grant No. SFRH/BD/81416/2011.
Submitted: 07/02/2017 Accepted: 17/04/2017

