










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAnálise Psicológica
versão impressa ISSN 0870-8231
Aná. Psicológica vol.32 no.3 Lisboa set. 2014
https://doi.org/10.14417/ap.835
Ethnic minorities’ and immigrants’ therapeutic (non)adherence: What is the role of social and cultural contexts?
Susana Sofia Monteiro Mourão* / Sónia Gomes da Costa Figueira Bernardes*
* ISCTE – Instituto Universitário de Lisboa, Centro de Investigação e Intervenção Social (CIS-IUL)
ABSTRACT
Immigrants and ethnic minorities have been identified as vulnerable groups in health, in general, and in what concerns therapeutic non-adherence (TA) in particular; i.e., (not)following health-care providers’ therapeutic recommendations. The general aim of this paper is presenting a literature review of immigrants’/ethnic minorities’ TA determinants. We will start by highlighting the reasons as to why immigrants’/ethnic minorities’ therapeutic (non)adherence should be a topic of concern. Then, we will present a review of the main determinants of immigrants’/ethnic minorities’TA, at different levels of analysis (e.g., broad structural level; social and community networks; material and social conditions) and emphasize that non-adherence among immigrants/ethnic minorities is mostly non-intentional, seeing as how it is associated with issues such as: low socio-economic conditions, language barriers and cultural mismatches. Finally, we will highlight the role of health-care providers in tackling this health-related problem and reflect about the importance of promoting development and training of health-care providers’ multicultural abilities.
Key-words: Therapeutic adherence, Determinants of (non)adherence, Immigrants, Ethnic minorities.
RESUMO
Os imigrantes e as minorias étnicas têm sido identificados como grupos vulneráveis na área da saúde, em geral, e no que diz respeito à (não)adesão terapêutica, em particular, i.e., (não)seguimento das recomendações dos profissionais de saúde. O objetivo geral deste artigo é o de apresentar uma revisão de literatura sobre os determinantes da (não)adesão terapêutica de imigrantes e minorias étnicas. Inicialmente, destacar-se-ão os motivos pelos quais a (não)adesão terapêutica de imigrantes/minorias étnicas poderá ser considerada como um tema relevante. Seguidamente, apresentar-se-á uma revisão sobre os principais determinantes da (não)adesão de imigrantes/minorias étnicas, em diferentes níveis de análise (e.g., estrutural; redes sociais e comunitárias; condições materiais e sociais) e destacar-se-á que a não-adesão entre os imigrantes/minorias étnicas é sobretudo não-intencional, por se encontrar associada a questões como: condições socioeconómicas desfavoráveis, barreiras linguísticas, desen contros culturais. Finalmente, salientar-se-á o papel dos profissionais de saúde na resolução deste problema relacionado com a saúde e reflectir-se-á sobre a importância de promover o desenvolvimento e a formação de competências multiculturais por estes profissionais.
Palavras-chave: Adesão terapêutica, Determinantes de (não)adesão, Imigrantes, Minorias étnicas.
INTRODUCTION
Imagine that you are living in a foreign country and you attend a medical appointment. When you enter the health-care facilities, you feel completely lost: you cannot understand the written information; the doctor tells you about the benefits of a specific diet, but she/he mentions food that you have never eaten and that you do not recognize; she/he prescribes you pills that are not approved in your country of origin. In these circumstances, you don’t feel very prone to complying with the doctor’s recommendations. But, why? And what are the implications of your non-adherence? Who (else) could advise or help you?
This example illustrates how immigrants and ethnic minorities can be considered vulnerable groups in health, in general, and therapeutic non-adherence (TA), in particular. The general aim of this paper is to present a literature review of immigrants’/ethnic minorities’ TA determinants. This literature review was based on a search for papers published after 2000, which showed a combination of keywords “treatment/therapeutic/medication adherence” and “immigrants/immigration”. This search was conducted in several databases, namely: Psycarticles, Pubmed, B-on, Scielo and Google Scholar.
In this paper, we will start by reflecting on the reasons as to why immigrants’/ethnic minorities’ therapeutic (non)adherence should be a topic of concern, then present its major determinants, and finally, we will highlight the role of health-care providers in tackling this health-related problem.
WHY IMMIGRANTS/ETHNIC MINORITIES ARE CONSIDERED VULNERABLE GROUPS IN HEALTH?
Several studies conducted in Portugal have identified immigrants/ethnic minorities as vulnerable groups in health, mainly for two reasons. First, some above mentioned barriers to accessing and using health services, such as: communication problems, due to language difficulties (Andrade, 2008; Dias, Severo, & Barros, 2008; Fonseca & Silva, 2010; Rosa, 2007; Silva & Martingo, 2007; Sousa, 2006) or different cultural meanings for the same health-related words (Moleiro, Silva, Rodrigues, & Borges, 2009; Silva & Martingo, 2007); negative behaviors observed in health-care providers, including discrimination (Dias, Rocha & Horta, 2009; Moleiro et al., 2009; Rosa, 2007) and poor knowledge about immigrants’ rights (Dias et al., 2009); the health services’ organization, including administrative barriers, difficulties in scheduling medical appointments (Andrade, 2008; Dias et al., 2009; Fonseca & Silva, 2010), or a lot of time waiting for consultations (Andrade, 2008; Dias et al., 2009; Fonseca & Silva, 2010; Gonçalves, Dias, Luck, Fernandes, & Cabral, 2003; Rosa, 2007; Sousa, 2006). Some of these barriers (e.g., communication problems) were also identified in some international studies related to immigrants’/ethnic minorities’ health (e.g., Mendoza, 2009; Schwarzwald, 2005).
Second, most immigrants/ethnic minorities often have a low socio-economic status, which can hamper their access to health services or have a negative impact on their state of health (Gurung, 2006; Jolly & Reeves, 2005; McKay, Macintyre, & Ellaway, 2003; Straub, 2012). These difficulties are identified in both national and international studies and cover issues such as: unemployment or precarious labor (Flores, Abreu, & Tomany-Korman, 2005; Javier, Huffman, Mendoza, & Wise, 2009; Machado et al., 2007); poor housing conditions (Andrade, 2008; Bäckström, 2009; Fonseca & Silva, 2010; Machado et al., 2007; Matos, Gonçalves, & Gaspar, 2004); social isolation (Andrade, 2008; Dias et al., 2009; Matos et al., 2004; Mendoza, 2009) or separation from family and significant others (Andrade, 2008; Dias et al., 2009); unstable condition in the host country (Dias et al., 2008; Gonçalves et al., 2003; Sousa, 2006). In some international contexts, not having health insurance may also be considered an important health related problem (Flores et al., 2005; Javier et al., 2009; Schwebel & Brezausek, 2009). Traditionally, all these conditions can increase health disparities (Jolly & Reeves, 2005; McKay et al., 2003; Mendoza, 2009).
The previous studies allow us to understand the general impact of migration in health, framing the main determinants that may contribute to immigrants’ and ethnic minorities’ vulnerability in this area. Nevertheless, their authors seem to report essentially to the concepts of “Access to and Use of Health Services”, which are more closely related with using or not the services and with how people manage the supplied resources (e.g., Travassos & Martins, 2004). Instead of focusing on immigrants’/ethnic minorities’ patterns of use of health care services, we will focus exclusively on a far less studied topic, especially in our national context – immigrants’/ethnic minorities’ TA.
WHAT IS THERAPEUTIC (NON)ADHERENCE AND WHY SHOULD WE WORRY ABOUT IT?
When we think about TA, most of us associate it with drug intake. Nevertheless, TA can be considered as a more embracing concept (e.g., Dunbar-Jacob, Schlenk, & McCall, 2012), also including following health-care providers’ recommendations related to health behaviors and lifestyle changes (e.g., diet recommendations) (Bosworth, Weinberger, & Oddone, 2006; Straub, 2012). But, why is it so important to focus on (non)adherence behaviors?
Poor TA is common and has important costs for individuals but also to health-care services and society. Poor TA is generally related with individuals’ worse general health status and illness progression, and with higher rates of disease complications and recurrent hospitalizations (e.g., Levensky & O’Donohue, 2006; Rodríguez-Gómez & Salas-Serrano, 2006). Consequently, health-care services report higher (unnecessary) tangible costs with drugs and consultations (Dunbar-Jacob et al., 2012), health-care providers are more likely to consider their work undervalued (Rodríguez-Gómez & Salas Serrano, 2006) and the effectiveness of pharmacological research can be compromised (McNicholas, 2012). Finally, since it is associated with work absenteeism, poor TA has considerable costs in terms of productivity (e.g., Bosworth et al., 2006; Dunbar-Jacob et al., 2012). Thus, we deem it important to try to improve TA, especially among members’ of vulnerable groups, such as immigrants and ethnic minorities.
HOW CAN WE ACCOUNT FOR IMMIGRANTS’AND ETHNIC MINORITIES’ (NON)ADHERENCE BEHAVIORS?
So far, most of the literature has emphasized intentional non-adherence, which assumes that people fail TA out of conscious decisions or lack of motivation (Dunbar-Jacob et al., 2012). In fact, so far most of the socio-cognitive theoretical models that have been used to understand TA behavior (change), tend to focus on individuals, neglecting their wider contexts, and argue that TA behaviors are essentially deliberate actions, which imply previous intention/motivation (e.g., Martin, Haskard-Zolnierek, & DiMatteo, 2010). However, and although there is much less research about it (Dunbar-Jacob et al., 2012), non-intentional non-adherence seems to be more relevant to account for immigrants’ and ethnic minorities’ TA behaviors. Why? Mostly because these have been associated with low socio-economic conditions (e.g., Ferguson & Scarlett-Ferguson, 2006), language barriers and cultural differences (e.g., Cheng & Walter, 2006; Dunbar-Jacob et al., 2012; Horne, 2007); particularly when health-care services are organized to serve the dominant culture (Gurung, 2006). Thus, among these social minority groups, contextual variables seem to acquire more significance in accounting for TA than individual characteristics.
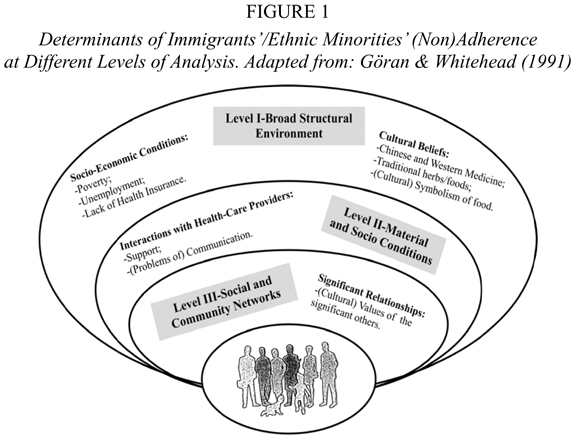
Moreover, social contexts may exert their influence over immigrants’ and ethnic minorities’ TA at different levels of analysis (e.g., Göran & Whitehead, 1991), namely, through the broad structural environment (e.g., SES and culture), material and social conditions (e.g., relation with health-care services) and social and community networks (e.g., family and significant others) (see Figure 1). Complex interactions between factors of different levels of analysis most often shape (non)adherence behaviors. For example, the mismatch between the cultural values of the patient and the doctor may have a strong impact on the quality of their interpersonal relationship. Nevertheless, and for the sake of clarity, in the following lines we will provide examples of determinants of immigrants/ethnic minorities’ non-adherence behaviors for each level of analysis separately.
The Role of Socio-Economic and Cultural Contexts
Socio-economic conditions and TA (see Figure 1-Level I). As referred previously, socio-economic conditions tend to have a large impact on health status, especially because it can limit the access to material and social resources that are important in promoting and maintaining health (Gurung, 2006; Marmot, 2004; Straub, 2012; Taylor, Repetti, & Seeman, 1997).
If socio-economic conditions have been shown to have a large impact on health status, they apparently also influence individuals’ TA behaviors (Bosworth et al., 2006; Levensky & O’Donohue, 2006; Martin et al., 2010). Immigrants and ethnic minorities often have low SES (Gurung, 2006; Straub, 2012) and non-adherence among these groups has been related to poverty (Colby, Wang, Chhabra, & Pérez-Escamilla, 2012; Tijerina, 2006, 2009) and unemployment (Vissman, Young, Wilkin, & Rhodes, 2013). How does this happen?
In some cases, poor TA occurs because of the high costs of drugs or recommended diet (e.g., hemodialysis treatment, which presupposes a specific diet) (Tijerina, 2006, 2009). In other cases, poor TA is related to lack of transportation to the health-care services (e.g., Vissman et al., 2011) and, in some countries, with lack of health insurance (e.g., Consedine, 2011).
In short, immigrants and ethnic minorities, by often having low SES, face barriers to both accessing the health-care services and, even when the access is granted, to complying with health-care professionals’ treatment recommendations.
Cultural beliefs and TA (see Figure 1-Level I). Different cultural groups may have different cultural beliefs and this mismatch can influence TA. For example, cultural concepts of health or illness linked to Traditional Chinese Medicine are different from Western Medicine – physical and mental health are considered to be a part of an unique concept as opposed to a dualistic mind-body representation, respectively (Gurung, 2006). According to this, a study conducted with Chinese Americans with diabetes has found that they prefer to control their disease with traditional herbs or foods and not use recommended pharmacological treatments (Chun & Chesla, 2004). Nevertheless, some authors warn about potential interactions between traditional methods and pharmacological treatments, describing that it may influence the course of medical regimen (e.g., Rodríguez-Gómez & Salas-Serrano, 2006).
Furthermore, a study conducted with Pakistani immigrants from Norway has concluded that they have a negative attitude towards some pharmacological treatments, namely related to generic drugs, which they believe could be associated with counterfeit products (Hakonsen & Toverud, 2011). Thus, their previous beliefs may influence their adherence to the prescribed generic drugs.
The examples above are essentially related to pharmacological regimens. However, different cultural concepts may also be important when sticking to diet recommendations (Bosworth et al., 2006; Gurung, 2006), as we mentioned in our first example. Immigrants with diseases that require dietary restrictions (e.g., diabetes) reported difficulties in adapting diet recommendations to their cultural beliefs (e.g., Chun & Chesla, 2004). Some of them highlighted the cultural symbolism of social gathering, where food abundance is a signal of quality of life. But how can family and significant others help manage these difficulties and contribute to a higher adherence among immigrants/ethnic minorities? Are they always a good influence?
The Role of Significant Relationships
The association between social relationships and health has been well-documented (House, Landis, & Umberson, 2004). Some researchers have emphasized the role played by social support groups and the influence of significant others to this relationship (e.g., House et al., 2004). These factors also seem to be relevant to immigrants’ and ethnic minorities’ (non)adherence.
Several studies conducted with immigrants have found that people who perceived emotional (e.g., reinforcement) and/or practical/technical (e.g., help to control a specific diet) support by their family (e.g., Griva et al., 2013), friends or other patients (e.g., Vissman et al., 2011) were more prone to be adherent (see Figure 1-Level III).
However, social relationships may also have their negative side, especially when cultural values of the significant others contrast with health-care providers’ recommendations or with the general cultural values of the host country (see Figure 1-Level III). For example, a study conducted with New Zealand Chinese citizens have found that they felt stigmatized when taking their psychiatric medications near their Chinese friends, who they believed were more discriminatory of people with mental illnesses than Western people were (Wang & Henning, 2010). On the other hand, a study conducted with Chinese, Malay and Indian immigrants in Singapore, treated by hemodialysis, has indicated that they felt social pressure to eat contra-indicated food, which influenced their adherence to the prescribed diet (Griva et al., 2013). Thus, it seems important that families and close relationships are aware of their potential influence in order to try to minimize their negative impact on TA. But what is the role of health-care providers in this scenario, considering their “expertise”?
The Role of Interaction with Health-Care Providers
Interactions between ethnic minorities/immigrants and health-care providers seem to play a major role on TA, which is considered an important determinant of (non)adherence (see Figure 1-Level II). For example, support from health-care providers was related to better TA of some immigrant groups (Colby et al., 2012; Vissman et al., 2011). Other immigrants stated that people who have negative feelings towards their doctors do not adhere to certain kinds of medication. In this case, they described that health-care providers did not know how to treat them, apart from prescribing drugs. Thus, the majority of them visited Chinese doctors, who shared their geographical background and who were able to speak their language (Wang & Henning, 2010). What can be learned from these examples? What are the similarities with our first example?
In both examples, the relationship between patient and health-care professional is embedded in a wider context, including the intervenients’ cultural backgrounds, which may be similar or not (Erger & Marelich, 2004). Thus, health-care providers’ communication skills and multicultural abilities seem to have a relevant impact on immigrants’ and ethnic minorities’ TA.
Communication and TA: More than different languages (see Figure 1-Level II). An effective communication allows health-care providers to understand patients’ symptoms and it is also useful to convey information about disease/treatment, in a way that could be applied (Martin et al., 2010; Straub, 2012). Thus, it is not surprising that communication can influence TA, especially considering that immigrants and ethnic minorities may not speak the same language as health-care providers and, consequently, may not understand what is explained to them (Gurung, 2006; Rodríguez-Gómez & Salas-Serrano, 2006). In our first example, the difficulties aroused from the very start, with the unintelligible written information in the health-care services.
In fact, language difficulties have been identified as the main communication problem related to immigrants’ non-adherence (e.g., Griva et al., 2013; Hakonsen & Toverud, 2011; Vissman et al., 2011). Besides this, some authors (e.g., Traylor, Schmittdiel, Uratsu, Mangione, & Subramanina, 2010) agree that language concordance between patients and health-care providers can be related with better TA, namely in Hispanic-Americans with diabetes.
However, verbal content is not the only dimension of communication. Have you ever had trouble understanding another person even though you were speaking the same language? In fact, communication has also latent cultural dimensions, which may not be directly expressed, but also have an effect on TA (Gurung, 2006). For example, some health-related words may have different meanings in different places across the world and this discrepancy could lead to non-adherence, especially if it is not accounted for by health-care providers (Gurung, 2006; Rodríguez-Gómez & Salas-Serrano, 2006).
Besides this, communication styles based on a mutual participation between patient and health-care providers, included on TA’s contemporary concepts (Bosworth et al., 2006), appear more easily adapted to Western developed countries. In some non-Western cultures, a sense of dependence on health-care providers appears to be well accepted (e.g., Hedemalm, Schaufelberger, & Ekman, 2010; McNicholas, 2012; Straub, 2012) and TA may be based on this.
In short, the relationship between health-care providers and immigrants/ethnic minorities appears to be a corner stone of TA among members of these social groups. That is probably why so many authors have been emphasizing the importance of promoting development and training of multicultural abilities among health-care professionals (e.g., Rodríguez-Gómez & Salas-Serrano, 2006).
Multicultural abilities: Cues for Intervention and Challenges for Further Research
Several of the above mentioned studies (e.g., Tucker et al., 2011) argued that it is essential that health professionals develop multicultural abilities. The focus of most interventions on this particular determinant of (non)adherence is probably related with its modifiable nature, especially when compared with some of the other mentioned determinants (e.g., socio-economic conditions).
Multicultural competencies are not necessarily related with being born or spending a long period of time in a certain country, but instead with an increase in socio-cultural consciousness (Rodríguez-Gómez & Salas-Serrano, 2006). In this particular case, it may be important that health-care providers have some knowledge about issues such as: general process of migration and some of the main problems in acculturation; real meaning that patients give to health-related words, because they may differ according to the origin and the host countries (Rodríguez-Gómez & Salas-Serrano, 2006); patients from low socio-economic conditions may not have access to some important material resources (e.g., difficulty to cook certain prescribed diets influenced by poor housing conditions) (Shapiro & Herivel, 2006); or certain cultural references from the patient’s country of origin, including the use of specific home drugs (Martin et al., 2010; Rodríguez-Gómez & Salas-Serrano, 2006). According to this, despite possible interactions between some traditional methods and pharmacological treatments, some researchers recommend trying to incorporate health traditional practices on medical regimens, whenever possible (McNicholas, 2012).
Considering the importance of an effective communication between immigrants/ethnic minorities and health-care providers, it may be also important that the written materials provided by health-care providers are culturally adapted. This intervention may imply not only its translation to the patient’s language, but also communicating some culture-specific attitudes or values (Martin et al., 2010; Rodríguez-Gómez & Salas-Serrano, 2006). According to this, health-care services may need to resort to translation or interpretation services, not neglecting certain patients’ rights, such as personal confidentiality (McNicholas, 2012).
Overall, and although it needs to be backed with empirical support, many authors suggest that to promote a better TA among immigrants and ethnic minorities health-care providers need to be non-judgmental, open and sensitive to eventual differences. To do so, some authors argue that it is essential that these professionals are trained on multicultural abilities right from their initial academic studies. Besides, the integration of formal cultural sensitivity training programs on health-care services (Rodríguez-Gómez & Salas-Serrano, 2006) may be relevant. It should be emphasized, however, that studies on the effectiveness of such intervention programs are still scarce (e.g., Dunbar-Jacob, Schlenk, & McCall, 2012; Levensky & O’Donohue, 2006; McNicholas, 2012), and constitute an important path for further research.
Let’s finally go back to our first example, imagining a culturally competent health-care service. You are living in a foreign country and you attend a medical appointment. You are a little nervous, because it is the first time that you need one, but this feeling is quickly overcome. All the written information is intelligible and written in several languages, so you can easily find the doctor’s room. At the beginning of the consultation, the doctor asks you to talk a bit about this (new) experience in the country, your expectations and your main fears. You get the feeling that she/he will help you, if needed be. That is a good thing, because your family and friends are so far away. Then, she/he tells you about the benefits of a specific diet, but asks you to think about typical foods from your country of origin that you may include in it. She/he also recommends you pills, and asks you if you know them. You tell him/her that they are not approved in your country of origin. She/he remembers she/he read some news about that, but regarding a different product, a counterfeit product. You leave the hospital thinking that these recommendations will be very beneficial to your health and you are willing to start the treatment right away.
REFERENCES
Andrade, I. J. M. (2008). Geografia da saúde da população imigrante na Área Metropolitana de Lisboa. Lisboa: ACIDI. [ Links ]
Bäckström, B. (2009). Saúde e imigrantes: As representações e as práticas sobre a saúde e a doença na comunidade Cabo-Verdiana em Lisboa. Lisboa: ACIDI. [ Links ]
Bosworth, H. B., Weinberger, M., & Oddone, E. Z. (2006). Introduction. In H. B. Bosworth, E. Z. Oddone, & M. Weinberger (Eds.), Patient treatment adherence: Concepts, interventions and measurement (pp. 3-12). New York: Routledge. [ Links ]
Cheng, J., & Walter, E. C. (2006). Nonadherence in Pediatrics. In H. B. Bosworth, E. Z. Oddone, & M. Weinberger (Eds.), Patient treatment adherence: Concepts, interventions and measurement (pp. 239-274). New York: Routledge. [ Links ]
Chun, K. M., & Chesla, C. A. (2004). Cultural issues in disease management for Chinese Americans with type 2 diabetes. Psychology & Health, 19(6), 767-785. doi: 10.1080/08870440410001722958 [ Links ]
Colby, J. A., Wang, F., Chhabra, J., & Pérez-Escamilla, R. (2012). Predictors of medication adherence in an urban Latino community with healthcare disparities. Journal of Immigrant and Minority Health, 14(4), 589-595. doi: 10.1007/s10903-011-9545-7. [ Links ]
Consedine, N. S. (2011). The demographic, system, and psychosocial origins of mammographic screening disparities: Prediction of initiating versus maintenance screening among immigrant and non-immigrant women. Journal of Immigrant and Minority Health, 14(4), 570-582. doi: 10.1007/s10903-011-9524-z [ Links ]
Dias, S. F., Rocha, C. F., & Horta, R. (2009). Saúde sexual e reprodutiva de mulheres imigrantes Africanas e Brasileiras. Lisboa: ACIDI. [ Links ]
Dias, S. F., Severo, M., & Barros, H. (2008). Determinants of health care utilization by immigrants in Portugal. BioMed Central Health Services Research, 8, 207-215. doi: 10.1186/1472-6963-8-207 [ Links ]
Dunbar-Jacob, J., Schlenk, E., & McCall, M. (2012). Patient adherence to treatment regimen. In A. Baum, T. A. Revenson, & J. Singer (Eds.), Handbook of health psychology (pp. 271-292). New York: Psychology Press. [ Links ]
Erger, J. S., & Marelich, W. D. (2004). Essay: Health care settings and their social dynamics. In W. D. Marelich & J. F. Erger (Eds.), The social psychology of health: Essays and readings (pp. 163-168). Thousand Oaks: Sage Publications. [ Links ]
Ferguson, K. E., & Scarlett-Ferguson, H. (2006). Skills training to promote patient adherence to treatments. In W. T. O’Donohue & E. R. Levensky (Eds.), Promoting treatment adherence: A practical handbook for health care providers (pp. 99-118). Thousand Oaks: Sage Publications.
Flores, G., Abreu, M., & Tomany-Korman, S. C. (2005). Limited English proficiency, primary language at home, and disparities in children’s health care: How language barriers are measured matters. Public Health Reports, 120, 418-430. Retrieved from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1497749/pdf/16025722.pdf
Fonseca, M. L., & Silva, S. (2010). Saúde e imigração: Utentes e serviços na área de influência do centro de saúde da Graça. Lisboa: ACIDI. [ Links ]
Gonçalves, A., Dias, S., Luck, M., Fernandes, M. J., & Cabral, J. (2003). Acesso aos cuidados de saúde de comunidades migrantes: Problemas e perspectivas de intervenção. Revista Portuguesa de Saúde Pública, 21, 55-64. Retrieved from: http://bibliobase.sermais.pt:8008/BiblioNET/upload/PDF/0215_Comunidades%20migrantes.pdf [ Links ]
Göran, D., & Whitehead, M. (1991). Policies and strategies to promote social equity in health (Background document to WHO – Strategy paper for Europe). Institute for Futures Studies. Retrieved from: http://whqlibdoc.who.int/euro/-1993/EUR_ICP_RPD414(2).pdf
Griva, K., Ng, H. J., Loei, J., Mooppil, N., McBain, H., & Newman, S. P. (2013). Managing treatment for end-stage renal disease – A qualitative study exploring cultural perspectives on facilitators and barriers to treatment adherence. Psychology & Health, 28(1), 13-29. doi: 10.1080/08870446.2012.703670
Gurung, R. A. R. (2006). Health psychology: A cultural approach. Belmont: Thomson Higher Education. [ Links ]
Hakonsen, H., & Tuverud, E. L. (2011). Special challenges for drug adherence following generic substitution in Pakistani immigrants living in Norway. European Journal of Clinical Pharmacology, 67(2), 193-201. doi: 10.1007/s00228-010-0960-9 [ Links ]
Hedemalm, A., Schaufelberger, M., & Ekman, I. (2010). Reported adherence and social support among immigrants compare to native Swedes. Journal of Immigrant and Minority Health, 12(1), 124-131. doi: 10.1007/s10903-009-9235-x [ Links ]
Horne, R. (2007). Adherence to treatment. In S. Ayers, A. Baum, C. McManus, S. Newman, K. Wallston, J. Weinman, & R. West (Eds.), Cambridge handbook of psychology, health and medicine (pp. 417-421). Cambridge: University Press. [ Links ]
House, J. S., Landis, K. R., & Umberson, D. (2004). Social relationships and health. In W. D. Marelich & J. F. Erger (Eds.), The social psychology of health: Essays and readings (pp. 237-246). Thousand Oaks: Sage Publications. [ Links ]
Javier, J. R., Huffman, L. C., Mendoza, F. S., & Wise, P. H. (2009). Children with special health care needs: How immigrant status is related to health care access, health care utilization, and health status. Matern Child Health, 14, 567-579. doi: 10.1007/s10995-009-0487-9 [ Links ]
Jolly, S., & Bridge, H. R. (2005). Gender and migration: Overview report. Bridge-Institute of United Kingdom: Development Studies. Retrieved from: http://www.bridge.ids.ac.uk/reports/cep-mig-or.pdf [ Links ]
Levensky, E. R., & O’Donohue, W. T. (2006). Patient adherence and non-adherence to treatments: An overview for health care providers. In W. T. O’Donohue & E. R. Levensky (Ed.), Promoting treatment adherence: A practical handbook for health care providers (pp. 3-14). Thousand Oaks: Sage Publications.
Machado, M. C., Santana, P., Carreiro, H., Nogueira, H., Barroso, R., & Dias, A. (2007). Cuidados de saúde materna e infantil a uma população de imigrantes. Revista Migrações, 1, 103-127. Retrieved from: http://www.oi.acidi.gov.pt/docs/Revista_1/migracoes1_art5.pdf [ Links ]
Matos, M. G., Gonçalves, A., & Gaspar, T. (2004). Adolescentes estrangeiros em Portugal: Uma questão de saúde. Psicologia, Saúde e Doenças, 5, 75-85. Retrieved from: http://www.scielo.oces.mctes.pt/pdf/psd/v5n1/v5n1a05.pdf [ Links ]
Marmot, M. (2004). The status syndrome: How social standing affects our health and longevity. New York: AHolt Paperback. [ Links ]
Martin, L. R., Haskard-Zolnierek, K. B., & DiMatteo, M. R. (2010). Health behavior change and treatment adherence: Evidence-based guidelines for improving healthcare. Oxford: University Press. [ Links ]
McKay, L., Macyntire, S., & Ellaway, A. (2003). Migration and health: A review of the international literature (MRC Social & Public Health Sciences Unit Occasional Paper-No 12). Glasgow: Medical Research Council. [ Links ]
McNicholas, F. (2012). To adhere or not, and what we can do to help. European Child & Adolescent Psychiatry, 21(12), 657-663. doi: 10.1007/s00787-012-0304-7 [ Links ]
Mendoza, F. S. (2009). Health disparities and children in immigrant families: A research agenda. Pediatrics, 124, 187-195. doi: 10.1542/peds.2009-1100F [ Links ]
Moleiro, C., Silva, A., Rodrigues, R., & Borges, V. (2009). Health and mental health needs and experiences of minority clients in Portugal. International Journal of Migration health and Social Care, 5, 15-24. doi: 10.1108/17479894200900003 [ Links ]
Rodríguez-Gómez, J. R., & Salas-Serrano, C. C. (2006). Treatment adherence in ethnic minorities: Particularities and alternatives. In W. T. O’Donohue & E. R. Levensky (Eds.), Promoting treatment adherence: A practical handbook for health care providers (pp. 393-400). Thousand Oaks: Sage Publications.
Rosa, C. F. S. C. (2007). Saúde mental em contexto migratório: Um estudo na região de Lisboa. Manuscripto não publicado, Universidade Aberta, Lisboa. Retrieved from: https://repositorioaberto.uab.pt/bitstream/10400.2/638/1/LC383.pdf [ Links ]
Schwarzwald, H. (2005). Illnesses among recently immigrated children. Seminars in pediatric infectious diseases, 16, 78-83. doi: 10.1053/j.spid.2005.12.003 [ Links ]
Schwebel, D. C., & Brezausek, C. M. (2009). Language acculturation and pediatric injury risk. Journal of Immigrant and Minority Health, 11, 168-173. doi: 10.1007/s10903-008-9158-y [ Links ]
Shapiro, R., & Herivel, M. (2006). In W. T. O’Donohue & E. R. Levensky (Ed.), Promoting treatment adherence: A practical handbook for health care providers (pp. 119-134). Thousand Oaks: Sage Publications.
Silva, A. C., & Martingo, C. (2007). Unidades de saúde amigas dos migrantes – Uma resposta ao desafio da multiculturalidade em Portugal. Revista Migrações, 1, 155-159. Retrieved from: http://www.oi.acidi.gov.pt/docs/Revista_1/migracoes1_art8.pdf
Sousa, J. E. X. F. (2006). Os imigrantes Ucranianos em Portugal e os cuidados de saúde. Porto: Alto-Comissariado para a Imigração e Minorias Étnicas [ACIME]. [ Links ]
Straub, R. O. (2012). Health psychology: A byopsychosocial approach. New York: Worth Publishers. [ Links ]
Taylor, S. E., Repetti, R. L., & Seeman, T. (1997). Health psychology: What is an unhealthy environment and how it gets under your skin? Annual Review of Psychology, 48, 411-447. doi: 10.1146/annurev.psych.48.1.411 [ Links ]
Tijerina, M. S. (2006). Psychosocial factors influencing Mexican-American women’s adherence with hemodialysis treatment. Social Work in Health Care, 43(1), 57-74. doi: 10.1300/J010v43n01_04
Tijerina, M. S. (2009). Mexican American women’s adherence to hemodialysis treatment: A social constructivist perspective. Social Work, 54(3), 232-242. doi: 10.1093/sw/54.3.232
Travassos, C., & Martins, M. (2004). Uma revisão sobre os conceitos de acesso e utilização de serviços de saúde. Cadernos de Saúde Pública, 20(2), 190-198. Retrieved from: http://www.scielosp.org/pdf/csp/v20s2/14.pdf [ Links ]
Traylor, A. H., Schmittdiel, J. A., Uratsu, C. S., Mangione, C. M., & Subramanian, U. (2010). Adherence to cardiovascular disease medications: Does patient-provider race/ethnicity and language concordance matter? Journal of General Internal Medicine, 25(11), 1172-1177. doi: 10.1007/s11606-010-1424-8 [ Links ]
Tucker, C. M., Marsiske, M., Rice, K. G., Nielson, J. J., & Herman, K. (2011). Patient-centered culturally sensitive health care: Model testing and refinement. Health Psychology, 30(3), 342-350. doi: 10.1037/a0022967 [ Links ]
Vissman, A. T., Young, A. M., Wilkin, A. M., & Rhodes, S. D. (2013). Correlates of HAART adherence among immigrant Latinos in the southeastern United States. Aids Care, 25, 356-363. doi: 10.1080/09540121.2012.701722 [ Links ]
Vissman, A. T., Hergenrather, K. C., Rojas, G., Langdon, S. E., Wilkin, A. M., & Rhodes, S. (2011). Applying the theory of planned behavior to explore HAART adherence among HIV-positive immigrant Latinos: Elicitation interview results. Patient Education and Counseling, 85(3), 454-460. doi: 10.1016/j.pec. 2010.12.004 [ Links ]
Wang, Y., & Henning, M. (2010). Bipolar disorder and medical adherence: A Chinese perspective. Asian Journal of Psychiatry, 3(1), 7-11. doi: 10.1016/j.ajp.2009.11.003 [ Links ]
A correspondência relativa a este artigo deverá ser enviada para: Susana Sofia Monteiro Mourão; ISCTE-Instituto Universitário de Lisboa, Centro de Investigação e Intervenção Social (CIS-IUL), Avª das Forças Armadas, 1649026 Lisboa; E-mail: Susana_Sofia_Mourao@iscte.pt
This work was supported by Fundação para a Ciência e Tecnologia (FCT): SFRH/BD/96783/2013.
Submissão: 23/02/2014 Aceitação: 20/06/2014

